

Exercise therapy and self-management support for individuals with multimorbidity: a randomized and controlled trial
- PMID: 40588675
- PMCID: PMC12443619
- DOI: 10.1038/s41591-025-03779-4
Exercise therapy and self-management support for individuals with multimorbidity: a randomized and controlled trial
Abstract
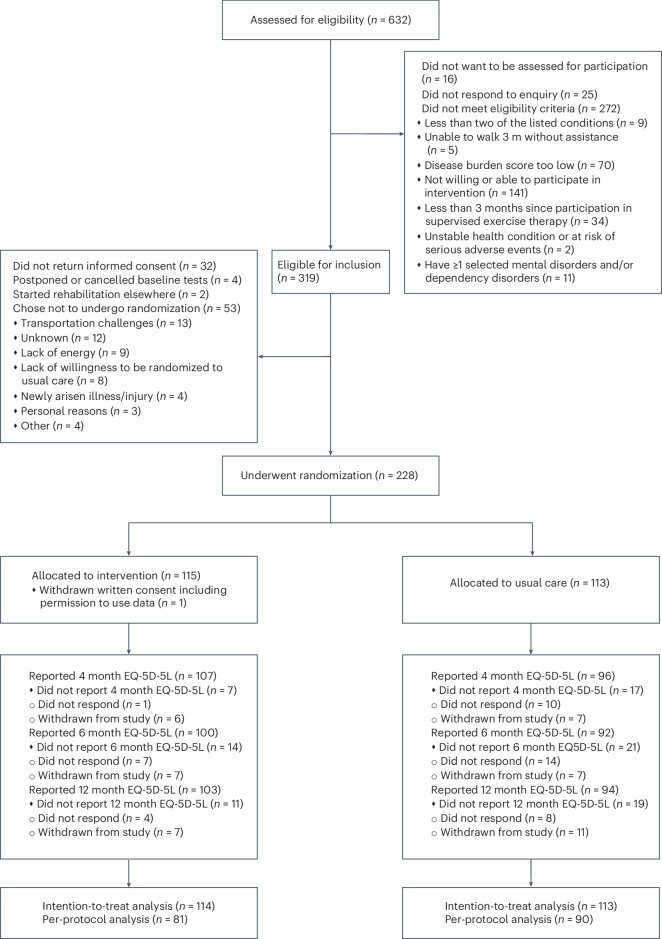
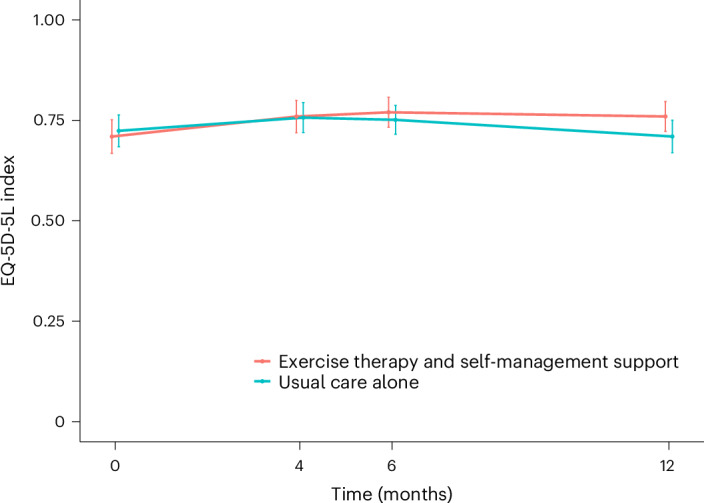
Despite increasing individual and societal burden, evidence for effective management strategies of multimorbidity is missing. Exercise therapy and self-management support are promising interventions, but their effect has not been evaluated. We hypothesized that exercise therapy and self-management support were superior to usual care alone in improving health-related quality of life (HRQoL) in individuals with multimorbidity. In this pragmatic multicenter, assessor-blinded randomized controlled trial (MOBILIZE), we enrolled 228 adult patients with two or more selected long-term conditions that limited their daily activities, but who were able to walk at least 3 meters without assistance, and who did not have unstable health conditions, life expectancy less than 12 months, or selected psychiatric conditions. Patients were randomized (1:1) to a 12 week personalized exercise therapy and self-management support program in addition to usual care or usual care alone. The primary outcome was HRQoL (using the EQ-5D-5L (European Quality of Life 5-dimensions 5-level version), ranging from -0.758 to 1, with higher scores being better) at 12 months, while secondary outcomes included functional performance (6 minute walk test and the 30 second chair-stand test), serious adverse events (SAEs), physical activity level (steps per day and minutes per day of at least light intensity measured with accelerometers), disease burden (Bayliss burden of illness measure), depression (Personal Health Questionnaire Depression Scale-8), anxiety (General Anxiety Disorder-7), self-efficacy (Self-Efficacy for Managing Chronic Disease scale), disability (12 item WHO Disability Assessment Schedule) and self-rated health (EQ-VAS (EuroQoL Visual Analog Scale)). In total, 197 of 228 participants (86%) completed the 12 month follow-up. On intention-to-treat analysis the exercise therapy and self-management support program had a statistically significantly greater effect on HRQoL than usual care alone (0.050 versus -0.014; adjusted mean difference, 0.064 points; 95% CI: 0.014-0.115). There were 36 and 48 SAEs in the exercise therapy and self-management group and usual care group, respectively (P = 0.388). Among the other secondary outcomes, only self-rated health was statistically significantly different between the groups (adjusted mean difference, 6.9 points; 95% CI: 1.8-12.1), in favor of the intervention group. In conclusion, this trial suggests that personalized exercise therapy and self-management support are more effective than usual care alone in improving health-related quality of life at 12 months in adults with multimorbidity, without compromising safety. The clinical relevance of the results remains unclear. ClinicalTrials.gov registration: NCT04645732 .
© 2025. The Author(s).
Conflict of interest statement
Competing interests: S.T.S. is co-founder of Good Life with Osteoarthritis in Denmark (GLA:D), a not-for-profit initiative hosted at University of Southern Denmark aimed at implementing clinical guidelines (exercise and self-management support) for individuals with osteoarthritis in clinical practice. All other authors have no competing interests.
Figures
References
-
- Head, A., Birkett, M., Fleming, K., Kypridemos, C. & O’Flaherty, M. Socioeconomic inequalities in accumulation of multimorbidity in England from 2019 to 2049: a microsimulation projection study. Lancet Public Health9, e231–e239 (2024). - PubMed
-
- Barnett, K. et al. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet380, 37–43 (2012). - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- 801790, MOBILIZE/EC | EU Framework Programme for Research and Innovation H2020 | H2020 Priority Excellent Science | H2020 European Research Council (H2020 Excellent Science - European Research Council)
- Exercise First/Region Sjælland (Region Zealand)
- N/A/Danske Fysioterapeuter (Association of Danish Physiotherapists)
LinkOut - more resources
Full Text Sources
Medical
