

Neoadjuvant Chemotherapy for Stage II Rectal Cancer Diagnosed in the Second Trimester of Pregnancy: A Case Report
- PMID: 40589557
- PMCID: PMC12206596
- DOI: 10.70352/scrj.cr.25-0208
Neoadjuvant Chemotherapy for Stage II Rectal Cancer Diagnosed in the Second Trimester of Pregnancy: A Case Report
Abstract
Introduction: The onset of colorectal cancer during pregnancy is rare, and no standard treatment has been established. In this report, we present the case of a woman with clinical stage II rectal cancer diagnosed in the second trimester, in which neoadjuvant chemotherapy was administered, followed by delivery once fetal development was sufficiently advanced, and surgery was performed afterward.
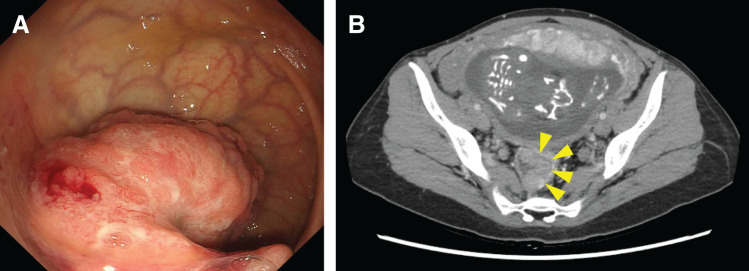
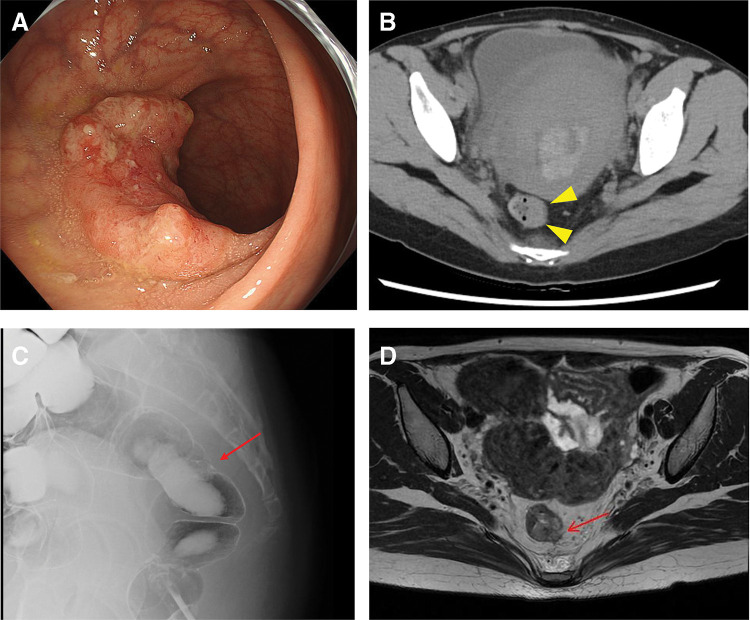
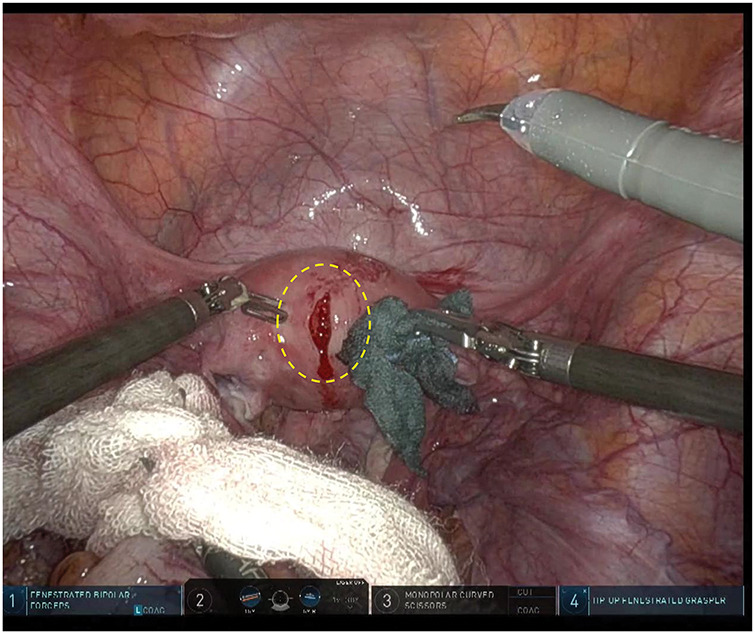
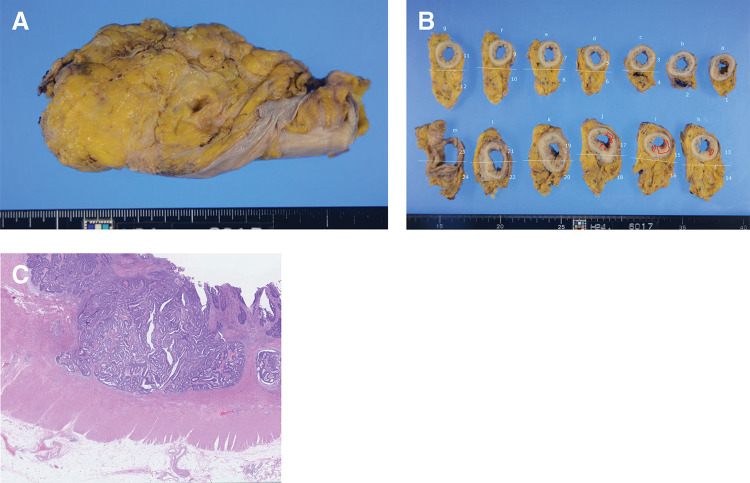
Case presentation: The patient was a 36-year-old woman at 22 weeks of gestation. Sigmoidoscopy was performed for hematochezia, which revealed a semicircular type 2 tumor in the rectum. A biopsy confirmed the presence of adenocarcinoma. A thorough systemic examination revealed no lymph nodes or distant metastases. After discussing the risks and benefits with the patient, her family, a pediatrician, and an obstetrician, we decided to administer neoadjuvant chemotherapy. The plan was to deliver the fetus after it had adequately developed and then perform radical surgery for rectal cancer after delivery. Neoadjuvant chemotherapy comprised 4 courses of the modified FOLFOX6 regimen, including leucovorin calcium (folinic acid), fluorouracil, and oxaliplatin. The patient had a vaginal delivery at 35 weeks and 5 days of gestation, 23 days after the last chemotherapy dose. The newborn was healthy with no congenital anomalies. On the 27th day after delivery, a robot-assisted low anterior resection of the rectum was performed. The pathological findings revealed rectal cancer located above the peritoneal reflection, ypT2N0M0, and ypStage I. The patient recovered well and was discharged 12 days after surgery. At the time of writing, both the mother and child are doing well, with no evidence of recurrence 6 months after surgery.
Conclusions: In cases of colorectal cancer during pregnancy, it is important to select a treatment plan that considers the site and stage of the tumor, number of weeks of pregnancy, and conditions of the fetus and mother. Even in cases of clinical stage II colorectal cancer diagnosed during the second trimester, where immediate surgery is not feasible, neoadjuvant chemotherapy can be considered a viable treatment option.
Keywords: case report; colorectal cancer; neoadjuvant chemotherapy; pregnancy; second trimester.
© 2025 The Author(s). Published by Japan Surgical Society.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Postoperative adjuvant chemotherapy in rectal cancer operated for cure.Cochrane Database Syst Rev. 2012 Mar 14;2012(3):CD004078. doi: 10.1002/14651858.CD004078.pub2. Cochrane Database Syst Rev. 2012. PMID: 22419291 Free PMC article.
-
Antiretrovirals for reducing the risk of mother-to-child transmission of HIV infection.Cochrane Database Syst Rev. 2011 Jul 6;(7):CD003510. doi: 10.1002/14651858.CD003510.pub3. Cochrane Database Syst Rev. 2011. PMID: 21735394
-
Antiretrovirals for reducing the risk of mother-to-child transmission of HIV infection.Cochrane Database Syst Rev. 2007 Jan 24;(1):CD003510. doi: 10.1002/14651858.CD003510.pub2. Cochrane Database Syst Rev. 2007. Update in: Cochrane Database Syst Rev. 2011 Jul 06;(7):CD003510. doi: 10.1002/14651858.CD003510.pub3. PMID: 17253490 Updated.
-
Chemotherapy for advanced gastric cancer.Cochrane Database Syst Rev. 2017 Aug 29;8(8):CD004064. doi: 10.1002/14651858.CD004064.pub4. Cochrane Database Syst Rev. 2017. PMID: 28850174 Free PMC article.
-
Impact of residual disease as a prognostic factor for survival in women with advanced epithelial ovarian cancer after primary surgery.Cochrane Database Syst Rev. 2022 Sep 26;9(9):CD015048. doi: 10.1002/14651858.CD015048.pub2. Cochrane Database Syst Rev. 2022. PMID: 36161421 Free PMC article.
References
-
- Girard RM, Lamarche J, Baillot R. Carcinoma of the colon associated with pregnancy: report of a case. Dis Colon Rectum 1981; 24: 473–5. - PubMed
-
- Walsh C, Fazio VW. Cancer of the colon, rectum, and anus during pregnancy. The surgeon’s perspective. Gastroenterol Clin North Am 1998; 27: 257–67. - PubMed
-
- Eibye S, Kjær SK, Mellemkjær L. Incidence of pregnancy-associated cancer in Denmark, 1977–2006. Obstet Gynecol 2013; 122: 608–17. - PubMed
-
- Bernstein MA, Madoff RD, Caushaj PF. Colon and rectal cancer in pregnancy. Dis Colon Rectum 1993; 36: 172–8. - PubMed
-
- Kocián P, de Haan J, Cardonick EH, et al. Management and outcome of colorectal cancer during pregnancy: report of 41 cases. Acta Chir Belg 2019; 119: 166–75. - PubMed