

Pembrolizumab plus chemotherapy with or without bevacizumab in East Asian participants with persistent, recurrent, or metastatic cervical cancer: results from KEYNOTE-826 final analysis
- PMID: 40590325
- PMCID: PMC12226315
- DOI: 10.3802/jgo.2025.36.e110
Pembrolizumab plus chemotherapy with or without bevacizumab in East Asian participants with persistent, recurrent, or metastatic cervical cancer: results from KEYNOTE-826 final analysis
Abstract
Objective: In the phase 3 KEYNOTE-826 study (NCT03635567), pembrolizumab plus chemotherapy with or without bevacizumab significantly improved progression-free survival (PFS) and overall survival (OS) in participants with persistent, recurrent, or metastatic cervical cancer. We report an exploratory analysis of outcomes for participants enrolled in East Asia based on the final analysis of KEYNOTE-826.
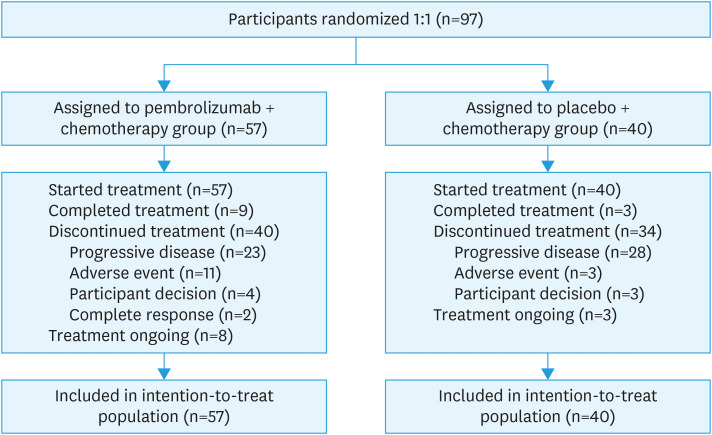
Methods: Participants were randomized 1:1 to receive pembrolizumab 200 mg or placebo every 3 weeks for up to 35 cycles. All participants received chemotherapy with paclitaxel and cisplatin or carboplatin for up to 6 cycles, and optionally received bevacizumab at the investigator's discretion. PFS and OS were dual primary endpoints.
Results: Ninety-seven participants from East Asia were enrolled in the intention-to-treat population. At data cutoff (October 3, 2022), in the intention-to-treat population, median PFS in the pembrolizumab plus chemotherapy and placebo plus chemotherapy groups was 18.0 and 10.4 months, respectively (hazard ratio [HR]=0.42; 95% confidence interval [CI]=0.23-0.77); median OS was not reached and 20.4 months, respectively (HR=0.53; 95% CI=0.28-0.99). In the programmed cell death ligand 1 combined positive score (CPS) ≥1 population, median PFS was 29.3 and 10.9 months, respectively (HR=0.36; 95% CI=0.19-0.68); median OS was not reached and 17.4 months, respectively (HR=0.43; 95% CI=0.22-0.86). The most common adverse events with pembrolizumab plus chemotherapy versus placebo plus chemotherapy were alopecia (75% vs. 68%) and anemia (67% vs. 65%).
Conclusion: These data support the use of pembrolizumab plus chemotherapy with or without bevacizumab for the treatment of persistent, recurrent, or metastatic cervical cancer in East Asian patients.
Trial registration: ClinicalTrials.gov Identifier: NCT03635567.
Keywords: Cervical Cancer; East Asia; Pembrolizumab.
© 2025. Asian Society of Gynecologic Oncology, Korean Society of Gynecologic Oncology, and Japan Society of Gynecologic Oncology.
Conflict of interest statement
Yong-Man Kim: Honoraria: Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA (MSD); Leadership role in other board, society, committee, or advocacy group: EAGOT, AOGIN, KGOG, KSMO.
Figures


References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–249. - PubMed
-
- Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA Cancer J Clin. 2024;74:12–49. - PubMed
-
- Chandra S, Goswami A, Mandal P. Molecular heterogeneity of cervical cancer among different ethnic/racial populations. J Racial Ethn Health Disparities. 2022;9:2441–2450. - PubMed
