

Validation of a risk-prediction model for pediatric post-discharge mortality after hospital admission for infection in Rwanda: A prospective cohort study
- PMID: 40591583
- PMCID: PMC12212559
- DOI: 10.1371/journal.pgph.0004606
Validation of a risk-prediction model for pediatric post-discharge mortality after hospital admission for infection in Rwanda: A prospective cohort study
Abstract
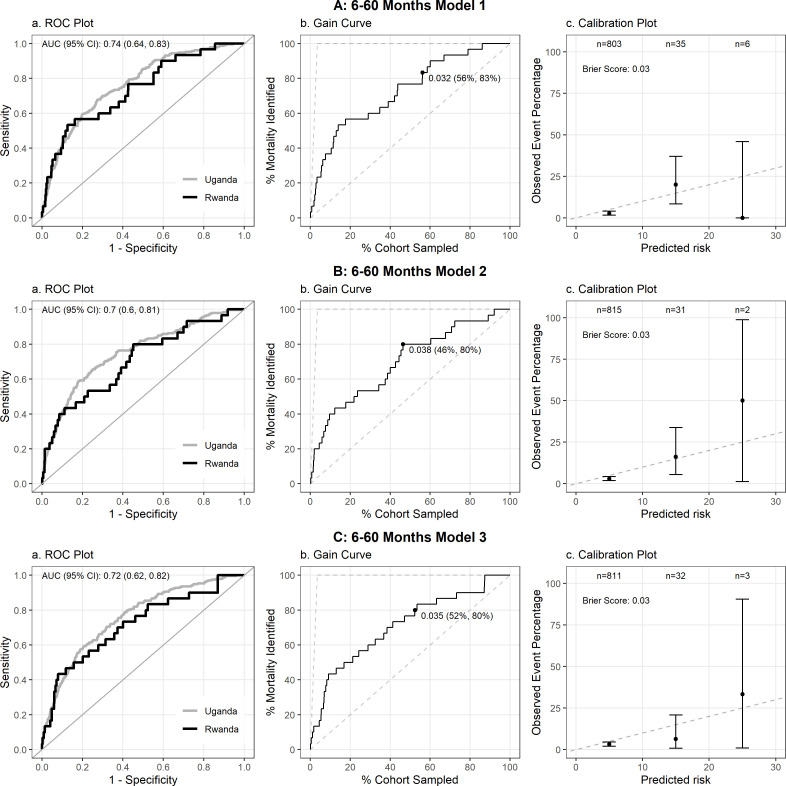
Mortality following hospital discharge remains a significant threat to child health, particularly in resource-limited settings. The Smart Discharges risk-prediction models use simple clinical, socio-behavioral, and point-of-care lab test variables to successfully predict children at the highest risk of death after hospital admission for infection to guide a risk-based approach to post-discharge care. In Rwanda, we externally validated five models derived from the prior Smart Discharges Uganda studies in a new cohort of children ages 0 days to 60 months admitted for suspected sepsis at two hospitals. We evaluated model performance using metrics including area under the receiver operating characteristic curve (AUROC), Brier score, and test characteristics (e.g., sensitivity, specificity). Performance was visualized through ROC and gain curves and calibration plots. Of 1218 total children (n = 413, Kigali; n = 805, Ruhengeri), 1161 lived to discharge (95.3%) and 1123 of those completed 6-month follow-up (96.7%). The overall rate of post-discharge mortality was 4.8% (n = 58). All five prediction models tested achieved an area under the receiver-operating curve (AUROC) greater than 0.7 (range 0.706 - 0.738). Low outcome rates resulted in moderately wide confidence intervals. Model degradation ranged from 1.1% to 7.7%, as determined by the percent reduction in AUROC between the internal validation of the original Ugandan cohort and the external Rwandan cohort. Calibration plots showed good calibration for all models at predicted probabilities below 10%. There were too few outcomes to assess calibration among those at the highest predicted risk levels. Discrimination was good with minimal degradation of the model despite low outcome rates. Future work to assess model calibration among the highest risk groups is required to ensure models are broadly generalizable to all children with suspected sepsis in Rwanda and in similar, resource-limited settings.
Copyright: © 2025 Hooft et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


References
-
- Umuhoza C, Hooft A, Uwiragiye E, Kornblith A, Wiens MO. Smart Discharges to improve post-discharge health outcomes in children in Rwanda - Smart Discharges - Study Protocols & Supplementary Materials. 2024. [cited 28 Aug 2024]. Available from: https://borealisdata.ca/dataset.xhtml?persistentId=doi:10.5683/SP3/NTNTZX - DOI
-
- United Nations. The Millennium Development Goals Report. 2015. doi: 978-92-1-101320-7
LinkOut - more resources
Full Text Sources
Miscellaneous