

Appraisal of multiple polygenic risk scores to estimate the risk of myocardial infarction and coronary artery lesions
- PMID: 40593158
- PMCID: PMC12216164
- DOI: 10.1038/s43856-025-00981-w
Appraisal of multiple polygenic risk scores to estimate the risk of myocardial infarction and coronary artery lesions
Abstract
Background: Polygenic risk scores (PRS) could help to identify individuals with a high genetic risk profile for coronary artery disease (CAD). We aimed to evaluate the association between previously reported PRS and myocardial infarction (MI) as well as the extent and recurrence of coronary artery lesions.
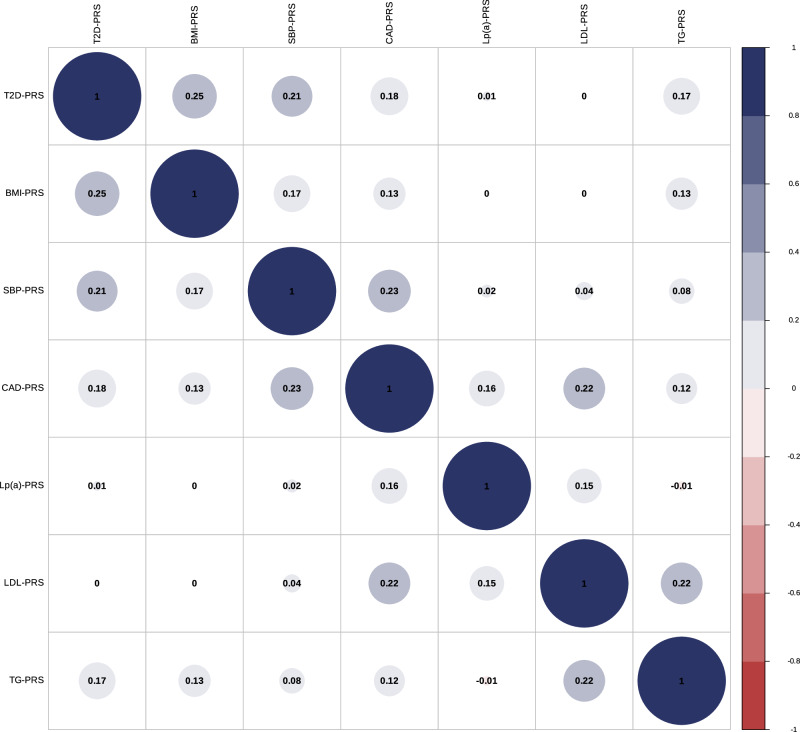
Methods: We validated previously reported CAD-PRS and 6 cardiovascular (CV) risk factors PRS (systolic blood pressure [SBP], type 2 diabetes [T2D], body-mass index [BMI], low-density lipoprotein cholesterol [LDL], triglycerides [TG], and lipoprotein-[a][Lp(a)]) in individuals of European ancestry from two Canadian population-based cohorts, the Canadian Longitudinal Study on Aging (CLSA, N = 24,599) and CARTaGENE (N = 26,806). Using a stepwise model, we determined an optimal combination of PRS to identify MI. We tested the selected PRS for association with the severity and recurrence of atherosclerotic CAD evaluated by coronary angiography in patients undergoing cardiac surgery (QUEBEC-ANGIO, N = 4108).
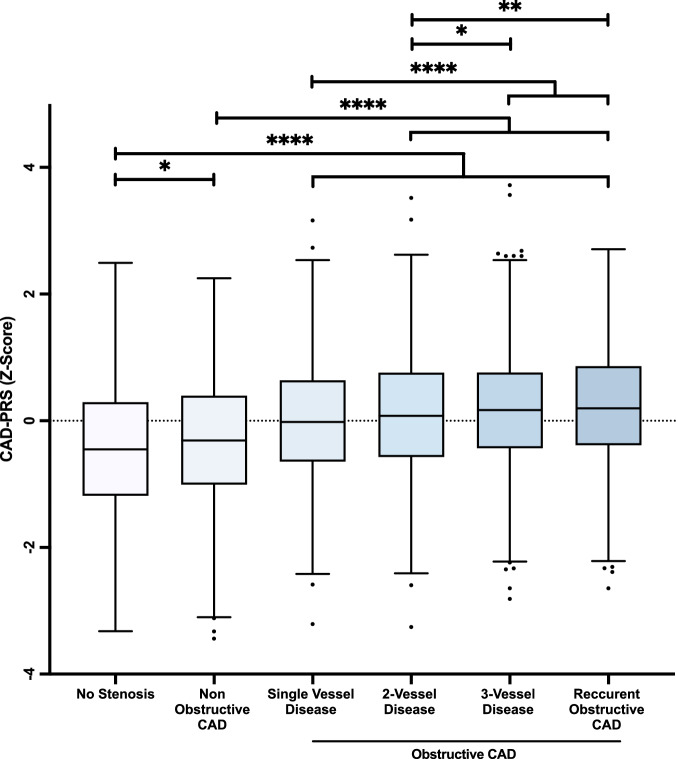
Results: We show that the CAD-PRS most strongly associated with MI has odds ratios per standard deviation increment of 1.75 [1.64-1.86] (P = 1.57E-70) in CLSA and 1.87 [1.73-2.03] (P = 3.06E-53) in CARTaGENE. In CLSA, the optimal model includes CAD-PRS, SBP-PRS, BMI-PRS, LDL-PRS, TG-PRS and Lp(a)-PRS. Adding these PRS increases modestly yet significantly the discriminative capacity when compared to traditional risk factors (difference of AUC = 0.025 [0.019-0.031] in CLSA, 0.018 [0.012-0.024] in CARTaGENE). In QUEBEC-ANGIO, the CAD-PRS is gradually and significantly associated with the extent and recurrence of CAD.
Conclusions: Screening multiple validated PRS may significantly improve genetic risk estimation of MI as well as the extent and recurrence of coronary artery lesions.
Plain language summary
Scores using common genetic (DNA) variations that can be measured in a blood sample have been developed to predict the risk of many diseases, including coronary heart disease (leading to heart attacks). In this study, we combined many of these scores to identify individuals who had a heart attack. We show that adding scores to known risk factors significantly improves prediction. We also show that some of these scores are associated with the level of obstruction in heart vessels measured during a specialized procedure. The use of these scores may improve the prediction of the risk of heart attack and obstruction of heart vessels.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare the following competing interests: B.J.A. is a consultant for Novartis and Silence Therapeutics and has received research funding from Pfizer and Ionis Pharmaceuticals. The other authors declare no competing interests. The opinions expressed in this manuscript are the authors’ own and do not reflect the views of the Canadian Longitudinal Study on Aging.
Figures

References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
