

Retrospective comparative study on efficacy and safety of different surgical procedures for pelvic organ prolapse
- PMID: 40593197
- PMCID: PMC12217270
- DOI: 10.1038/s41598-025-07878-7
Retrospective comparative study on efficacy and safety of different surgical procedures for pelvic organ prolapse
Abstract
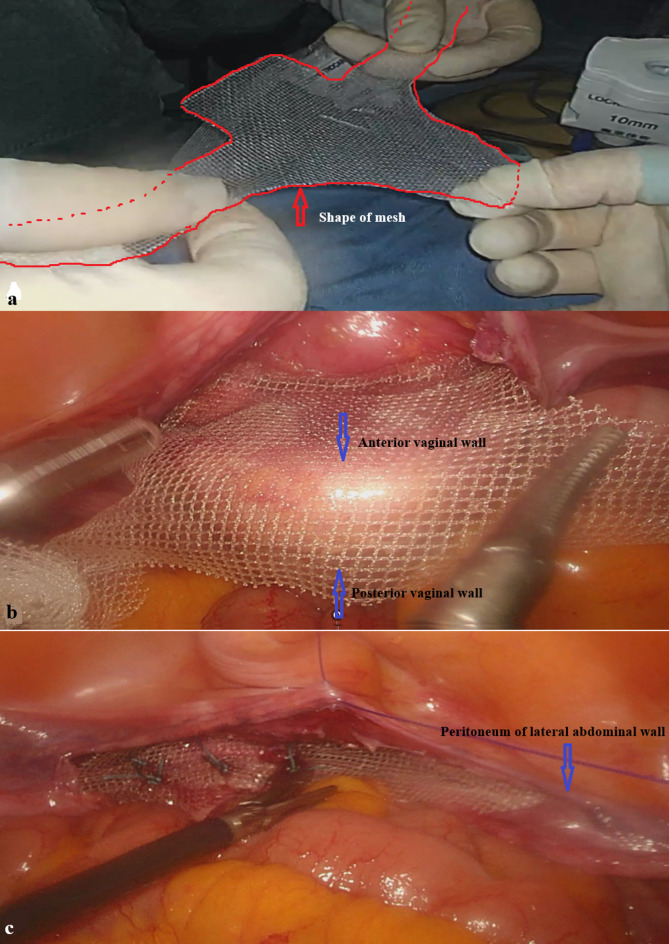
The aim of this retrospective study was to analyze the efficacy and safety of lateral abdominal wall suspension during surgery compared with traditional procedures in patients with pelvic organ prolapse without uterine preservation. Collect the data of patients with uterine and vaginal wall prolapse who underwent surgery from January 2022 to December 2023. All patients were divided into three groups according to different surgical procedures: Study Group (laparoscopic total hysterectomy + bilateral salpingectomy/oophorectomy + lateral abdominal wall suspension + posterior colporrhaphy), Control Group 1 (laparoscopic-assisted vaginal total hysterectomy + bilateral salpingectomy/bilateral oophorectomy + anterior and posterior colporrhaphy), and Control Group 2 (vaginal total hysterectomy + anterior and posterior colporrhaphy).Statistically analyze the clinical indicators and recurrence situations in different Groups. Patients in Study group exhibited significantly higher preoperative POP-Q staging for pelvic organ prolapse severity(P < 0.01), longer operative times(P = 0.01, P < 0.01), but significantly reduced intraoperative blood loss(P = 0.01, P < 0.01)and shorter postoperative urinary catheterization duration(P = 0.01, P < 0.01) compared to the other two groups. No differences were detected in postoperative infection, vaginal bleeding or duration of hospitalization(P > 0.05). However, stress incontinence in 1-year after operation has no difference between study group and control groups. Recurrence rates in Control Group 1 is higher than Study Group (P = 0.02), While, it has no difference between Study Group and Control Group 2. Lateral abdominal wall suspension, despite a longer operative duration, surpasses traditional surgeries in minimizing intraoperative blood loss, cutting down the time of postoperative urinary catheter retention, and lowering the postoperative recurrence rate. To firmly establish the long-term curative effects and safety of lateral abdominal wall suspension, future research with larger sample sizes and longer follow-up periods is essential.
Keywords: Laparoscopy; Lateral mesh suspension; Uterine prolapse.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethical approval: This study adopts a retrospective research approach. During the research process, no special interventions were implemented on the included patients. All patient data used have been strictly stripped of personal privacy and sensitive information. This includes removing patients’ names, ID numbers, contact information, specific home addresses,ensuring that it is impossible to trace back to individuals through the data. Informed consent was obtained from all individual participants included in this retrospective study. The study protocol was approved by the Institutional Review Board of Tianjin medical university second hospital (approval number:KY2025K097). All procedures and methods in this study were carried out in strict accordance with ethical standards, relevant guidelines, and national regulations.
Figures
Similar articles
-
Surgery for women with pelvic organ prolapse with or without stress urinary incontinence.Cochrane Database Syst Rev. 2018 Aug 19;8(8):CD013108. doi: 10.1002/14651858.CD013108. Cochrane Database Syst Rev. 2018. PMID: 30121956 Free PMC article.
-
Surgical management of pelvic organ prolapse in women.Cochrane Database Syst Rev. 2010 Apr 14;(4):CD004014. doi: 10.1002/14651858.CD004014.pub4. Cochrane Database Syst Rev. 2010. Update in: Cochrane Database Syst Rev. 2013 Apr 30;(4):CD004014. doi: 10.1002/14651858.CD004014.pub5. PMID: 20393938 Updated.
-
Surgery for women with posterior compartment prolapse.Cochrane Database Syst Rev. 2018 Mar 5;3(3):CD012975. doi: 10.1002/14651858.CD012975. Cochrane Database Syst Rev. 2018. PMID: 29502352 Free PMC article.
-
Surgery for women with apical vaginal prolapse.Cochrane Database Syst Rev. 2023 Jul 26;7(7):CD012376. doi: 10.1002/14651858.CD012376.pub2. Cochrane Database Syst Rev. 2023. PMID: 37493538 Free PMC article.
-
Abdominal and vaginal pelvic support with concomitant hysterectomy for uterovaginal pelvic prolapse: a comparative systematic review and meta-analysis.Int Urogynecol J. 2021 Aug;32(8):2021-2031. doi: 10.1007/s00192-021-04861-4. Epub 2021 May 29. Int Urogynecol J. 2021. PMID: 34050771
References
-
- Mezes, C. M. et al. Effect of vaginal prolapse repair and midurethral sling on urgency incontinence symptoms. Urogynecology (Phila)31(3), 250–257. 10.1097/SPV.0000000000001620 (2025). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
