

Clinical and functional outcomes of masquelet technique for treating Fracture-related Infections(FRIs) in shoulder girdle
- PMID: 40593306
- PMCID: PMC12215267
- DOI: 10.1038/s41598-025-08386-4
Clinical and functional outcomes of masquelet technique for treating Fracture-related Infections(FRIs) in shoulder girdle
Abstract
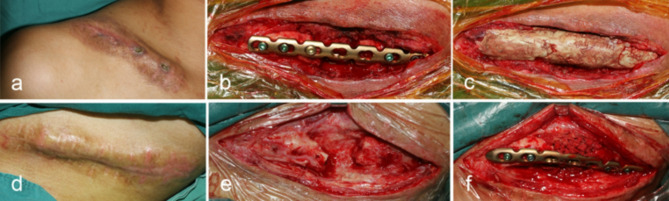
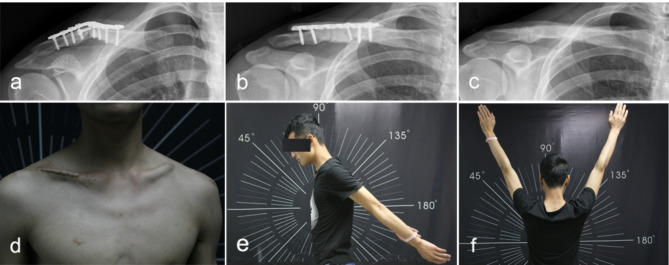
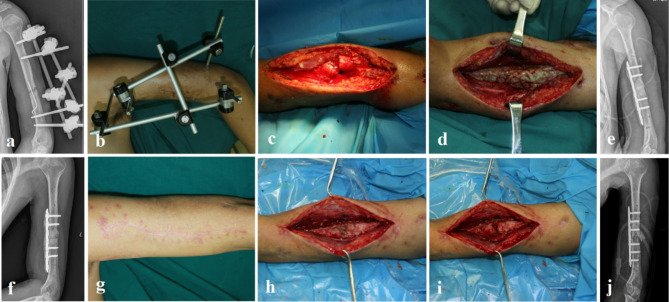
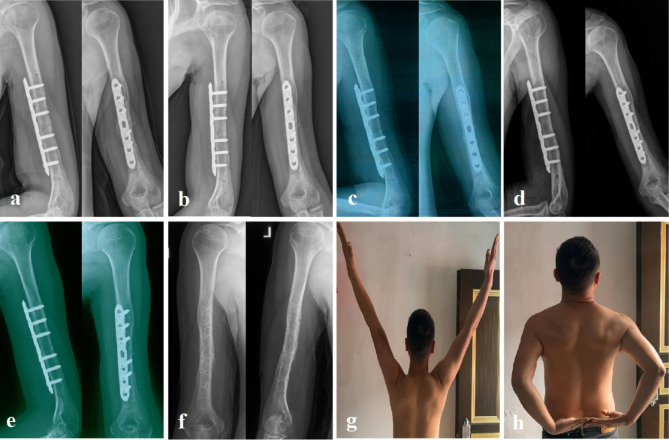
Structural and functional integrity pose a challenge for the treatment of fracture-related infections (FRI) in the shoulder girdle. The purpose of this study was to assess the clinical and functional outcomes of patients treated with the Masquelet technique. From January 2012 to January 2023, sixty-two consecutive adult patients with FRI in the shoulder girdle (8 in clavicle and 54 in humerus) were treated using this technique. This involved the use of antibiotic bone cement to fill the dead space after debridement, followed by staged bone grafting. Patients' outcomes, in terms of infection resolution, bone union, and the Disabilities of the Arm, Shoulder, and Hand (DASH) score, were retrospectively analyzed. The follow-up time was at least 2 years. The mean age was 45.52±14.01 years. The initial fracture was open in 16 patients (25.8%) and closed in 46 patients (74.2%), Staphylococcus aureus (21.0%) was the most common pathogen. Thirty-six patients with large bone defects had additional locking plates for internal fixation. All patients achieved bone consolidation after a median follow-up of 24 months (range: 24-72 months) after the second stage bone graft. Clinical bone healing occurred at 4 months in 56.5%, at 6 months in 29.0%, and at 9 months in 14.5%. Seven patients required additional revision surgery. Three of these patients underwent repeated debridement before grafting due to incomplete infection control, while four had recurrence after the second-stage bone graft and required repeat surgery. The average DASH scores showed a significant decrease at the final follow-up, from a mean of 47.37 before surgery to a mean of 13.31. Following univariate analysis, patient age, post-debridement internal fixation, and bone graft type were not associated with the need for additional revision. However, patients aged ≥ 60 years (p = 0.004) and those with prolonged infection duration (p=0.002) were more likely to experience poor functional outcomes. The Masquelet technique, though requiring a staged approach, achieved reliable infection control and bony union in shoulder girdle FRIs, with favorable functional outcomes. This staged technique provided advantages through the use of antibiotic-loaded cement spacers, enabling local antibiotic treatment, dead space management, and post-debridement internal fixation.
Keywords: Fracture-related infection; Function; Masquelet technique; Shoulder girdle.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: All the authors declare that there are no conflicts of interest. Ethical review statement: This study was approved by the Ethics Committee of Southwest Hospital Chongqing, China (No. KY201878). The informed consent was waived by the Ethics Committee of Southwest Hospital Chongqing, as this is an observational cohort study and personal information was de-identified.
Figures
Similar articles
-
Does Augmenting Irradiated Autografts With Free Vascularized Fibula Graft in Patients With Bone Loss From a Malignant Tumor Achieve Union, Function, and Complication Rate Comparably to Patients Without Bone Loss and Augmentation When Reconstructing Intercalary Resections in the Lower Extremity?Clin Orthop Relat Res. 2025 Jun 26. doi: 10.1097/CORR.0000000000003599. Online ahead of print. Clin Orthop Relat Res. 2025. PMID: 40569278
-
Management of Unique Complex Long Bone Fractures by Gunshot Injuries with Linear Rail System.Ann Afr Med. 2025 Jul 1;24(3):562-566. doi: 10.4103/aam.aam_143_23. Epub 2025 May 30. Ann Afr Med. 2025. PMID: 40445311 English, French.
-
Masquelet technique: myth or reality? A systematic review and meta-analysis.Injury. 2016 Dec;47 Suppl 6:S68-S76. doi: 10.1016/S0020-1383(16)30842-7. Injury. 2016. PMID: 28040090
-
Guided tissue regeneration for periodontal infra-bony defects.Cochrane Database Syst Rev. 2006 Apr 19;(2):CD001724. doi: 10.1002/14651858.CD001724.pub2. Cochrane Database Syst Rev. 2006. Update in: Cochrane Database Syst Rev. 2019 May 29;5:CD001724. doi: 10.1002/14651858.CD001724.pub3. PMID: 16625546 Updated.
-
Clinical and radiological outcomes of arthroscopic bony Bankart repair using the 'door-locking' technique: excellent bone healing with a low complication rate.J Shoulder Elbow Surg. 2025 Aug;34(8):e637-e644. doi: 10.1016/j.jse.2024.11.011. Epub 2025 Jan 3. J Shoulder Elbow Surg. 2025. PMID: 39756640
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
