

Enrichment of gut-derived metabolites in a Parkinson's disease subtype with REM sleep behavior disorder
- PMID: 40593920
- PMCID: PMC12219260
- DOI: 10.1038/s41531-025-01040-w
Enrichment of gut-derived metabolites in a Parkinson's disease subtype with REM sleep behavior disorder
Abstract
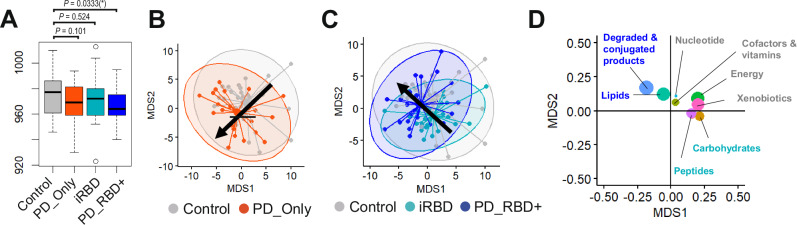
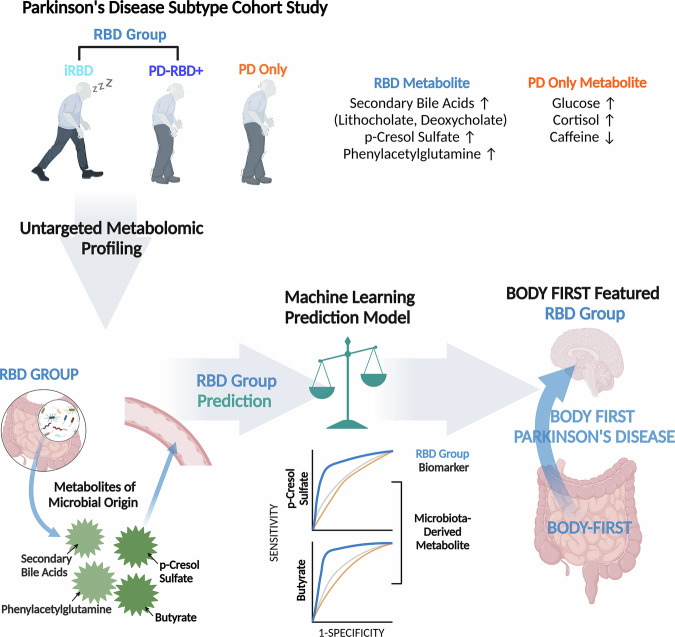
Recent reports indicate that Parkinson's disease (PD)-like changes in gut microbial signatures develop in idiopathic REM sleep behavior disorder (iRBD), a prodrome of α-synucleinopathies. However, <50% of PD cases exhibit RBD at onset, underscoring PD's heterogeneity. Using untargeted metabolomics, plasma samples from PD patients with and without RBD, iRBD subjects, and healthy controls were analyzed to characterize the metabolic differences in PD patients with and without RBD. Metabolomic analysis revealed the enrichment of gut microbial-origin metabolites, such as secondary bile acids and p-cresol sulfate, in PD patients with RBD, while metabolites linked to neuropsychiatric diseases were elevated in PD patients without RBD. Additionally, our prediction that p-cresol sulfate, enriched in the RBD groups with a gut microbial origin, crosses the blood-brain barrier, suggests a potential mechanistic link between gut microbial dysbiosis, iRBD, and PD with RBD. Our study elucidates the heterogeneous nature of PD subtypes.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures



References
-
- Morris, H. R., Spillantini, M. G., Sue, C. M. & Williams-Gray, C. H. The pathogenesis of Parkinson’s disease. Lancet403, 293–304 (2024). - PubMed
-
- Berg, D. et al. Prodromal Parkinson disease subtypes - key to understanding heterogeneity. Nat. Rev. Neurol.17, 349–361 (2021). - PubMed
-
- Braak, H. et al. Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol. Aging24, 197–211 (2003). - PubMed
-
- Horsager, J. et al. Brain-first versus body-first Parkinson’s disease: a multimodal imaging case-control study. Brain143, 3077–3088 (2020). - PubMed
-
- Cersosimo, M. G. & Benarroch, E. E. Pathological correlates of gastrointestinal dysfunction in Parkinson’s disease. Neurobiol. Dis.46, 559–564 (2012). - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
