

Correction of syndesmotic malreduction following fixation flexibilization
- PMID: 40593952
- PMCID: PMC12218112
- DOI: 10.1038/s41598-025-04117-x
Correction of syndesmotic malreduction following fixation flexibilization
Abstract
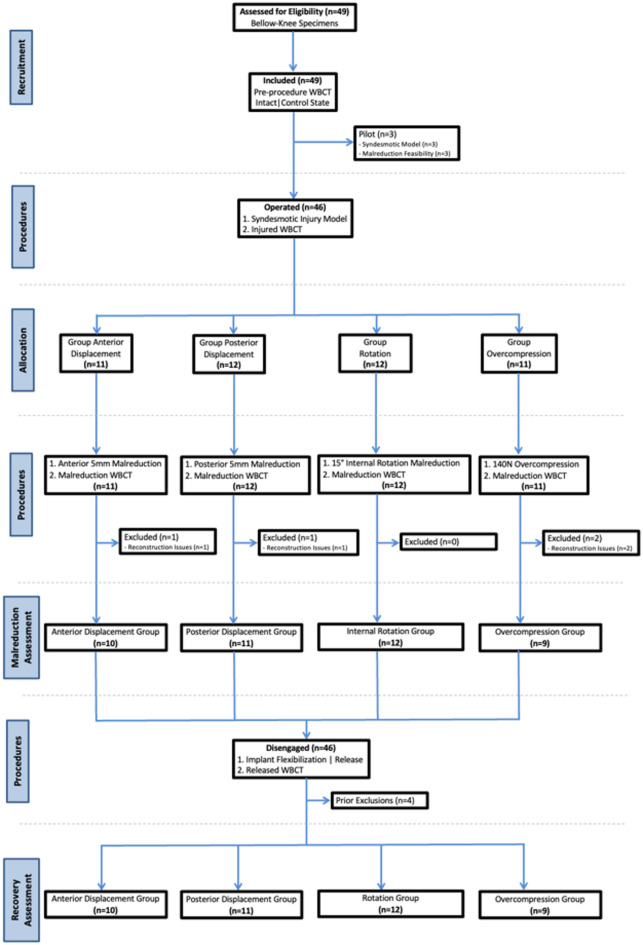
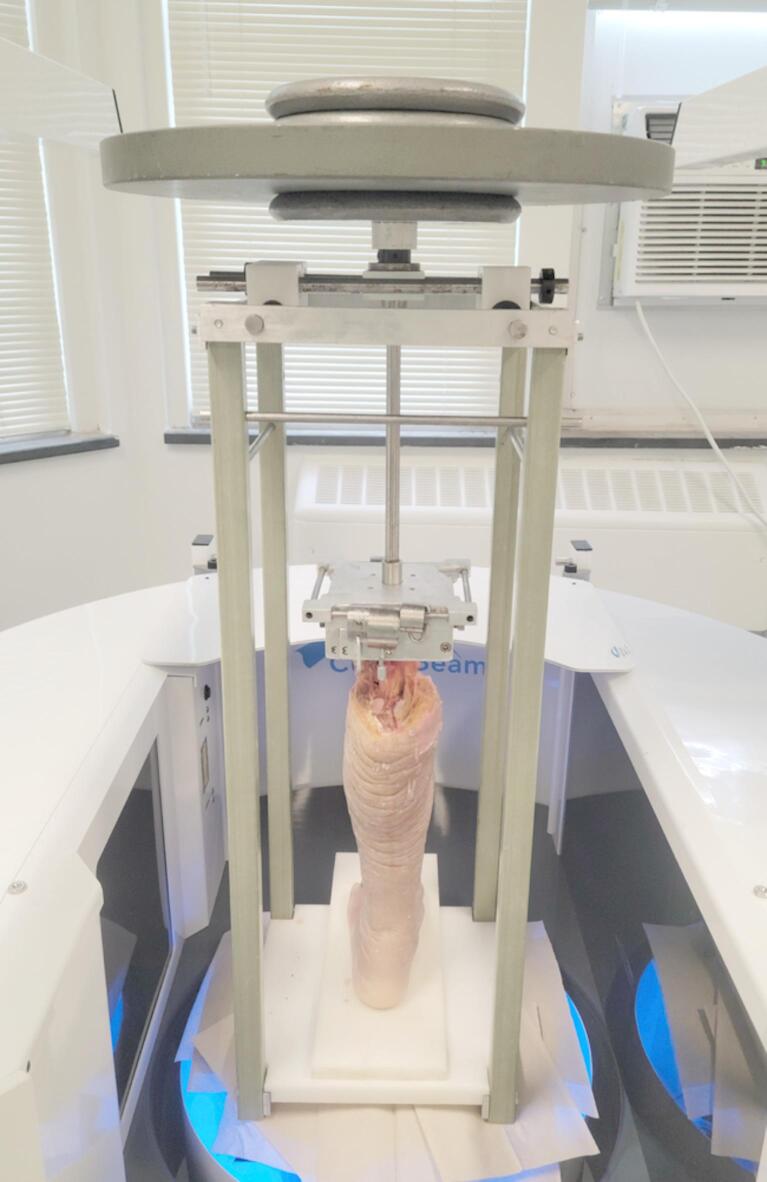
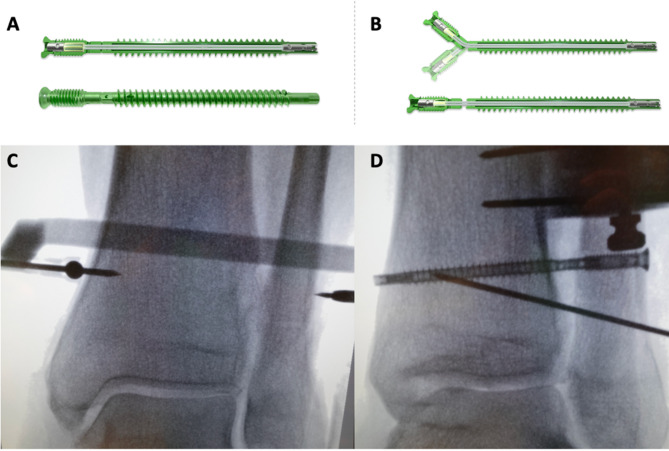
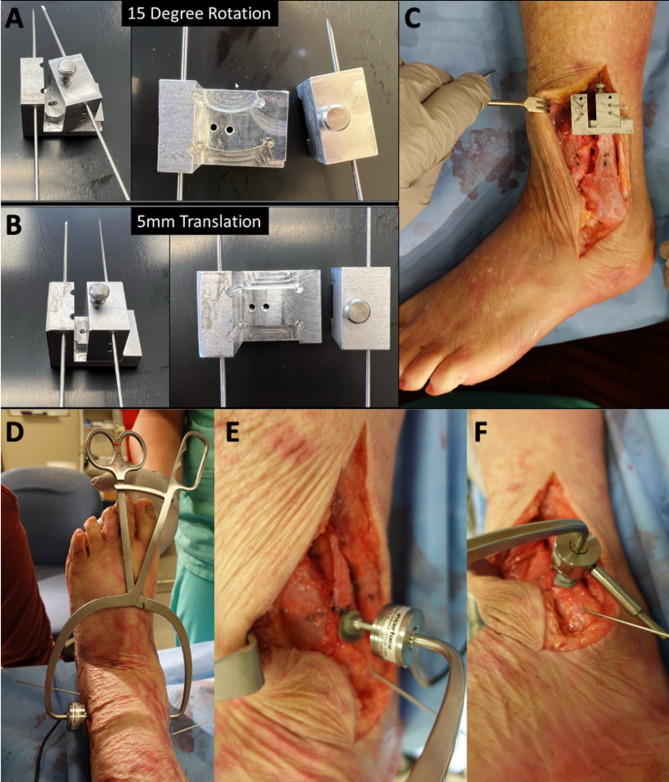
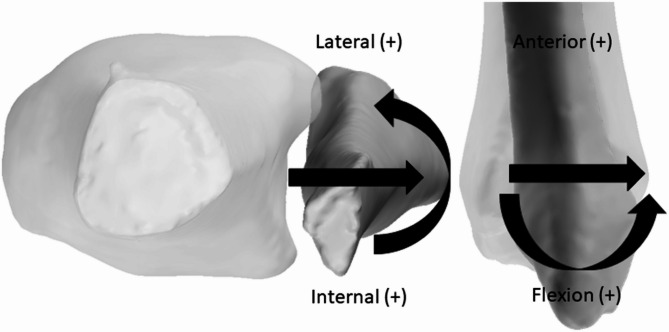
Prior studies showed the potential of a rigid fixation, such as a trans-syndesmotic screw, to produce tibiofibular malreduction. Flexible implants, although capable of allowing forgiveness, may not provide sufficient stability for all injury patterns. To assess the malreduction forgiveness of a two-phase syndesmotic device that is designed to transition from a rigid screw construct to a flexible suture-type. Cadaveric specimens were loaded in a frame under four conditions: native (control), syndesmotic instability (injured), malreduced with engaged syndesmotic device (malreduced), and post-disengagement (disengaged). The malreduction targets were 5 mm anterior displacement, 5 mm posterior displacement, 15° of rotation, and 140 N over-compressed. Fixation was performed with a single device 20 mm proximal to the ankle, manually disengaged to allow semi-constrained motion of the syndesmosis. Weightbearing Computed Tomography (WBCT) scans were obtained, and anatomic axes of the tibia and fibula extracted to calculate tibiofibular joint position with an established orthogonal system. A total of 42 specimens were included and allocated in the four groups. Anterior and posterior malreduction demonstrated 2.50 mm (SD: ±1.37 mm) and 5.04 mm (SD: ±2.23 mm) of average malreduction. The disengaged condition resulted in average recovery of 1.79 mm (95%CI: 0.72|2.85; p = 0.0034; 72% recovery) and 1.69 mm (95%CI: 0.09|3.28; p = 0.0006; 33% recovery) toward the control position, for anterior and posterior malreduction, respectively. Rotational malreduction demonstrated 2.44° (SD: ±2.09°) of average rotational malreduction, with 1.98° (95%CI: -0.13°|4.09°; p = 0.0707; 81%) of recovery. Over-compression specimens showed average medial translation of 0.89 mm (SD: ±1.10 mm), with 0.74 mm (95%CI: 0.05|1.51; p = 0.0128; 82%) of recovery when disengaged. The two-phase syndesmotic device was able to allow partial malreduction recovery in different scenarios after transitioning to the flexible state. The use of this implant might mitigate potential surgical tibiofibular malreductions while providing the mechanical and clinical advantages of both rigid and flexible devices. Level V. Controlled laboratory study.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The study was partially funded by a Paragon 28 grant. Implants used in this study were also from Paragon 28.Individual Competing Interests: Nacime Salomao Barbachan Mansur, MD, PhDBrazilian Foot and Ankle Society: Board or committee memberAmerican Orthopaedic Foot and Ankle Society: Board or committee memberJohn Y Kwon, MDDJ Orthopaedics: IP royalties; Paid consultantMedline: IP royaltiesParagon 28: IP royalties; Paid consultantRestor3D: Paid consultantTrimed: IP royaltiesCesar De Cesar Netto, MD, PhDAmerican Orthopaedic Foot and Ankle Society: Board or committee memberCurveBeam: Paid consultant; Stock or stock OptionsFoot and Ankle International: Editorial or governing boardNextremity: Paid consultantOssio: Paid consultantParagon 28: IP royalties; Paid consultantWeightbearing CT International Study Group: Board or committee memberZimmer: Paid consultant The other authors have nothing to disclosure.All authors have completed the ICMJE uniform disclosure form (www.icmje.org/coi_disclosure) and declare no support from any organization for the submitted work; Other authors have no financial relationships with any organizations that might have an interest in the submitted work in the previous ten years; no other relationships or activities that could appear to have influenced the submitted work.
Figures


Similar articles
-
A systematic review of suture-button versus syndesmotic screw in the treatment of distal tibiofibular syndesmosis injury.BMC Musculoskelet Disord. 2017 Jul 4;18(1):286. doi: 10.1186/s12891-017-1645-7. BMC Musculoskelet Disord. 2017. PMID: 28676078 Free PMC article.
-
Assessing the Need for Additional Syndesmotic Stabilization in Open Reduction of the Posterior Malleolus: A Biomechanical Study.J Bone Joint Surg Am. 2025 Apr 17;107(12):1377-1385. doi: 10.2106/JBJS.23.01088. J Bone Joint Surg Am. 2025. PMID: 40245116 Free PMC article.
-
Mini Fragment and Small Fragment Screws are Comparable in Acute Syndesmotic Injury.J Foot Ankle Surg. 2025 Jul-Aug;64(4):367-371. doi: 10.1053/j.jfas.2025.01.003. Epub 2025 Jan 11. J Foot Ankle Surg. 2025. PMID: 39800110
-
Acute distal tibiofibular syndesmosis injury: a systematic review of suture-button versus syndesmotic screw repair.Int Orthop. 2012 Jun;36(6):1199-206. doi: 10.1007/s00264-012-1500-2. Epub 2012 Feb 9. Int Orthop. 2012. PMID: 22318415 Free PMC article.
-
A Cadaveric Study: Does Ankle Positioning Affect the Quality of Anatomic Syndesmosis Reduction?J Orthop Trauma. 2024 Aug 1;38(8):e307-e311. doi: 10.1097/BOT.0000000000002827. J Orthop Trauma. 2024. PMID: 39007668
References
-
- Harris, M. C. et al. Prospective results of the modified glide path technique for improved syndesmotic reduction during ankle fracture fixation. Foot Ankle Int.43 (7), 923–927. 10.1177/10711007221081868 (2022). - PubMed
-
- Veen, E. J. & Zuurmond, R. G. Mid-term results of ankle fractures with and without syndesmotic rupture. Foot Ankle Surg.21 (1), 30–36. 10.1016/j.fas.2014.09.001 (2015). - PubMed
-
- Hunt, K. J., Goeb, Y., Behn, A. W., Criswell, B. & Chou, L. Ankle joint contact loads and displacement with progressive syndesmotic injury. Foot Ankle Int.36 (9), 1095–1103. 10.1177/1071100715583456 (2015). - PubMed
-
- Goetz, J. E., Rungprai, C., Rudert, M. J., Warth, L. C. & Phisitkul, P. Screw fixation of the syndesmosis alters joint contact characteristics in an axially loaded cadaveric model. Foot Ankle Surg.25 (5), 594–600. 10.1016/j.fas.2018.05.003 (2019). - PubMed
-
- Miller, A. N., Barei, D. P., Iaquinto, J. M., Ledoux, W. R. & Beingessner, D. M. Iatrogenic syndesmosis malreduction via clamp and screw placement. J. Orthop. Trauma.27 (2), 100–106. 10.1097/BOT.0b013e31825197cb (2013). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
