

Surgical timing and approach for brainstem cavernous malformation warranting thorough preoperative evaluation
- PMID: 40594083
- PMCID: PMC12216782
- DOI: 10.1038/s41598-025-03722-0
Surgical timing and approach for brainstem cavernous malformation warranting thorough preoperative evaluation
Abstract
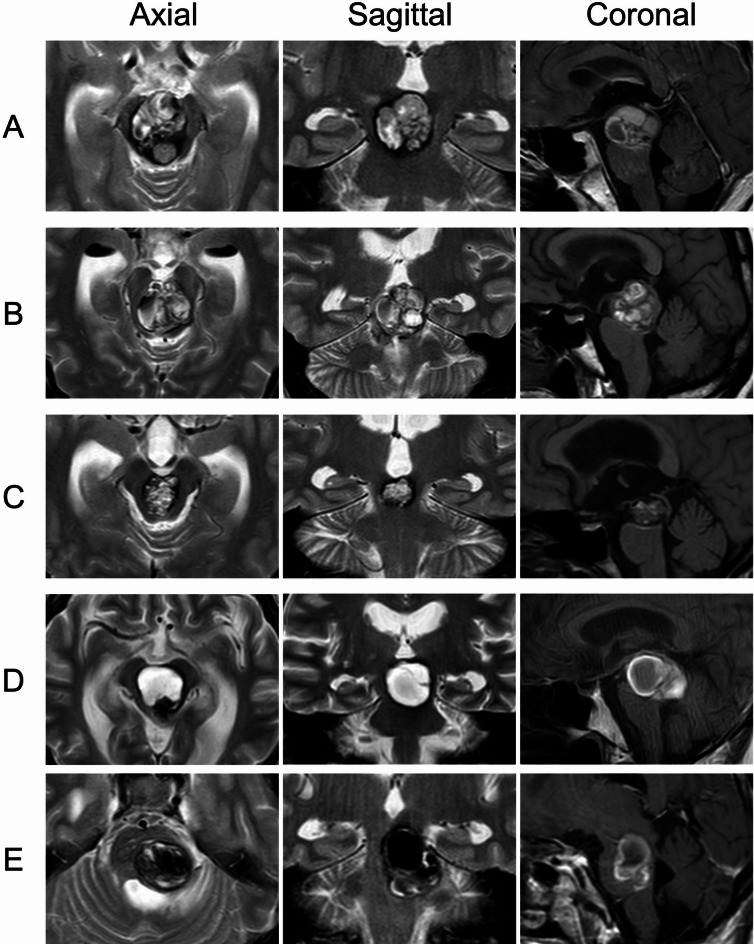
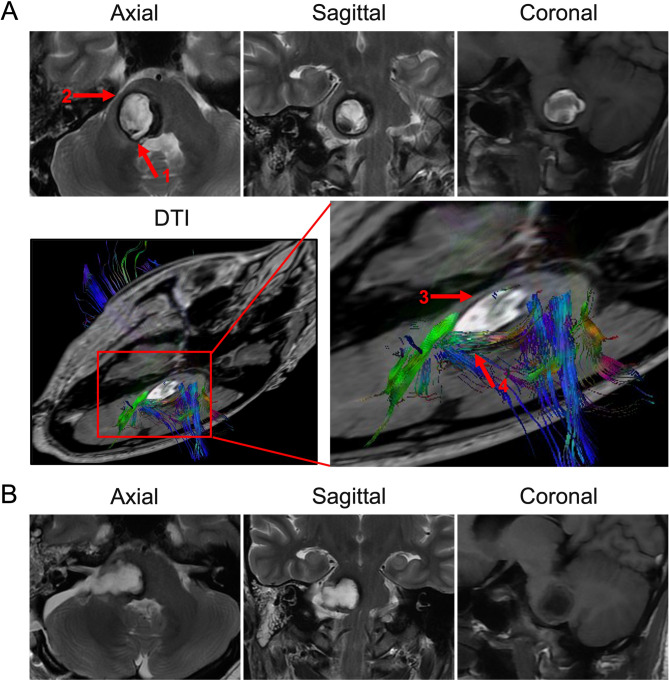
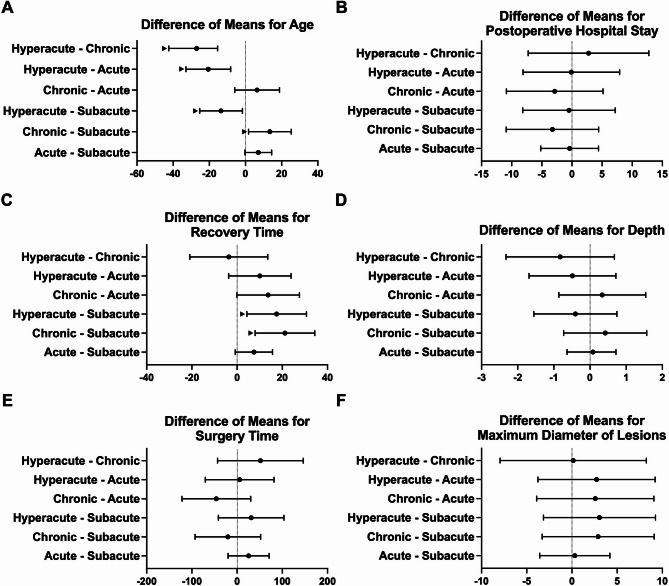
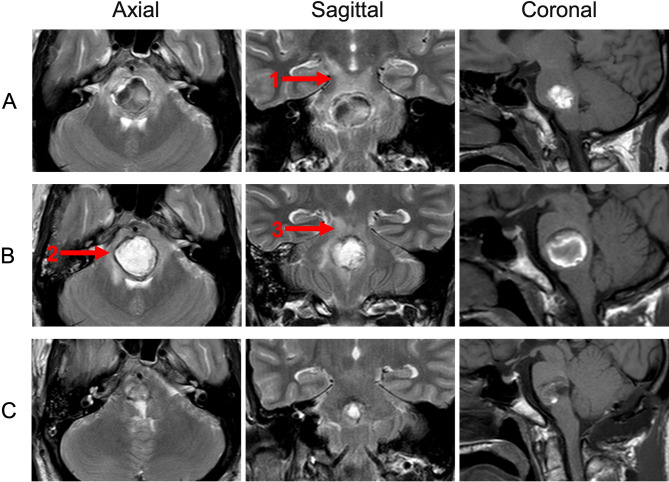
Hemorrhage from brainstem cavernous malformations (BSCMs) can cause severe neurological dysfunction. While surgery is effective, the optimal timing remains unclear. This retrospective study aims to identify the best timing for surgery after hemorrhage in BSCM patients. Data from patients who underwent surgery between 2012 and 2022 were analyzed. Patients were divided into groups with favorable and unfavorable outcomes based on their best post-treatment modified Rankin Scale (mRS) scores. They were further categorized into four groups according to the timing of surgery after hemorrhage: hyperacute (≤ 7 days), acute (8-20 days), subacute (21-56 days), and chronic (> 56 days). Clinical characteristics, imaging findings, prognosis, and outcomes were compared between the groups. A total of 135 BSCM patients were included, with most lesions located in the pons. Surgical timing distribution was as follows: hyperacute phase (12 cases), acute phase (42 cases), subacute phase (69 cases), and chronic phase (12 cases). Of these, 113 patients had favorable outcomes. Statistical analysis revealed a significant difference in mRS scores between the four groups, with the most pronounced differences observed between the acute/subacute phases and the hyperacute/chronic phases. In conclusion, performing surgery in the acute and subacute phases could improve neurological function in BSCM patients.
Keywords: Brainstem cavernous malformations; Outcome; Surgical resection; Surgical timing.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures
References
-
- <ISSVA-Classification-2018.pdf>.
MeSH terms
LinkOut - more resources
Full Text Sources
