

Impact of craniofacial skeletal characteristics on temporomandibular joint's articular disc position in temporomandibular disorders
- PMID: 40594311
- PMCID: PMC12214861
- DOI: 10.1038/s41598-025-04938-w
Impact of craniofacial skeletal characteristics on temporomandibular joint's articular disc position in temporomandibular disorders
Abstract
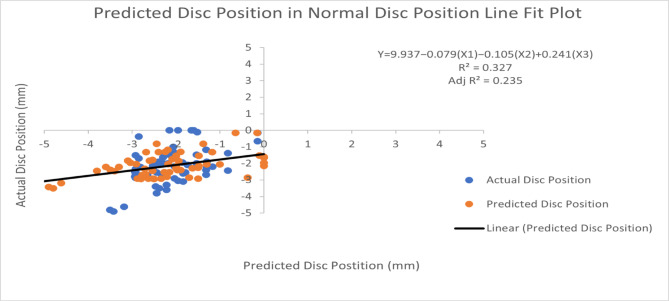
This retrospective study aims to: (1) determine whether craniofacial skeletal characteristics differ based on the type of temporomandibular joint (TMJ) disc displacement (DD); and (2) identify cephalometric variables that correlate with and predict articular disc position. A total of 294 joints corresponding to 147 female patients, aged 18 to 41 years, were included. Based on the criteria of DC/TMD and subsequently magnetic resonance imaging (MRI) findings, the joints were categorized into three groups: 1) bilateral normal disc position (BN), 2) disc displacement with reduction (DDR), and 3) disc displacement without reduction (DDWR). The lateral cephalograms were assessed, and twelve landmarks were marked on each radiograph, from which fifteen variables were derived. Cone beam computed tomography (CBCT) images were evaluated for joint spaces, glenoid fossa characteristics, and condylar inclination. One-way ANOVA and post-hoc Tukey tests were used to compare variables across groups. Bivariate Pearson correlation analysis was conducted to assess relationships between glenoid fossa characteristics, disc position, condylar position, and skeletal morphology. Multiple linear regression (MLR) was applied to determine cephalometric predictors of disc position. Significant differences were observed in joint spaces, condylar inclination, and fossa morphology across the three groups. ANB, FMA, y-axis, gonial angle, and ramus height showed significant correlations with disc position. MLR demonstrated that FMA, ramus height, and articular angle were the strongest predictors of DD, particularly in DDWR, with an explanatory power of 55% (R2 = 0.55, p < 0.001). Craniofacial morphology plays a key role in the pathophysiology of DD. Patients with a steeper mandibular plane (higher FMA) and reduced ramus height were more prone to DDWR. These findings highlight the importance of cephalometric evaluation in assessing TMD and predicting disc position.
Keywords: Cone beam computed tomography; Craniofacial morphology; Disc displacement; Internal derangement; Magnetic resonance imaging; Temporomandibular disorders; Temporomandibular joint.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethical approval: This retrospective study was ethically approved by the Stomatological Hospital of Xi’an Jiaotong University Medical Ethics Committee under the ethical approval number: 2024-XJKQIEC-KY-QT-0035-002. All methods were carried out in accordance with relevant guidelines and regulations. Informed consent was obtained from all subjects.
Figures







Similar articles
-
Cone-Beam Computed Tomography as a Diagnostic Tool for TMJ Morphological Alterations in Disc Displacement.Int Dent J. 2025 Jul 29;75(5):100908. doi: 10.1016/j.identj.2025.100908. Online ahead of print. Int Dent J. 2025. PMID: 40738007 Free PMC article.
-
The relationship between the articular disc in magnetic resonance imaging and the condyle in cone beam computed tomography: A retrospective study.J Stomatol Oral Maxillofac Surg. 2024 Sep;125(12 Suppl 2):101940. doi: 10.1016/j.jormas.2024.101940. Epub 2024 Jun 8. J Stomatol Oral Maxillofac Surg. 2024. PMID: 38857693
-
Age and Gender-related Morphometric Assessment and Degenerative Changes of Temporomandibular Joint in Symptomatic Subjects and Controls using Cone Beam Computed Tomography (CBCT): A Comparative Analysis.Curr Med Imaging. 2024;20:e15734056248617. doi: 10.2174/0115734056248617231002110417. Curr Med Imaging. 2024. PMID: 38389339
-
Recommendations for standard criteria for the positional and morphological evaluation of temporomandibular joint osseous structures using cone-beam CT: a systematic review.Eur Radiol. 2024 May;34(5):3126-3140. doi: 10.1007/s00330-023-10248-4. Epub 2023 Oct 25. Eur Radiol. 2024. PMID: 37878020 Free PMC article.
-
Changes in temporomandibular joint morphology in class II patients treated with fixed mandibular repositioning and evaluated through 3D imaging: a systematic review.Orthod Craniofac Res. 2015 Nov;18(4):185-201. doi: 10.1111/ocr.12099. Epub 2015 Aug 11. Orthod Craniofac Res. 2015. PMID: 26260422
References
-
- Shu, C., Xiong, X., Huang, L. & Liu, Y. The relation of cephalometric features to internal derangements of the temporomandibular joint: A systematic review and meta-analysis of observational studies. Orthod. Craniofac. Res.24, 305–313. 10.1111/ocr.12454 (2021). - PubMed
-
- Valesan, L. F. et al. Prevalence of temporomandibular joint disorders: A systematic review and meta-analysis. Clin. Oral Investig.25, 441–453. 10.1007/s00784-020-03710-w (2021). - PubMed
-
- Flores-Mir, C., Nebbe, B., Heo, G. & Major, P. W. Longitudinal study of temporomandibular joint disc status and craniofacial growth. Am. J. Orthod. Dentofacial Orthop.130, 324–330. 10.1016/j.ajodo.2005.01.024 (2006). - PubMed
-
- Schiffman, E. et al. Diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and research applications: Recommendations of the international RDC/TMD consortium network* and orofacial pain special interest Group†. J. Oral Facial Pain Headache28, 6–27. 10.11607/jop.1151 (2014). - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
