

Preoperative chlorhexidine mouthwash can reduce the risk of postoperative pulmonary complications in elderly patients undergoing general anesthesia with endotracheal intubation
- PMID: 40594330
- PMCID: PMC12217547
- DOI: 10.1038/s41598-025-06417-8
Preoperative chlorhexidine mouthwash can reduce the risk of postoperative pulmonary complications in elderly patients undergoing general anesthesia with endotracheal intubation
Abstract
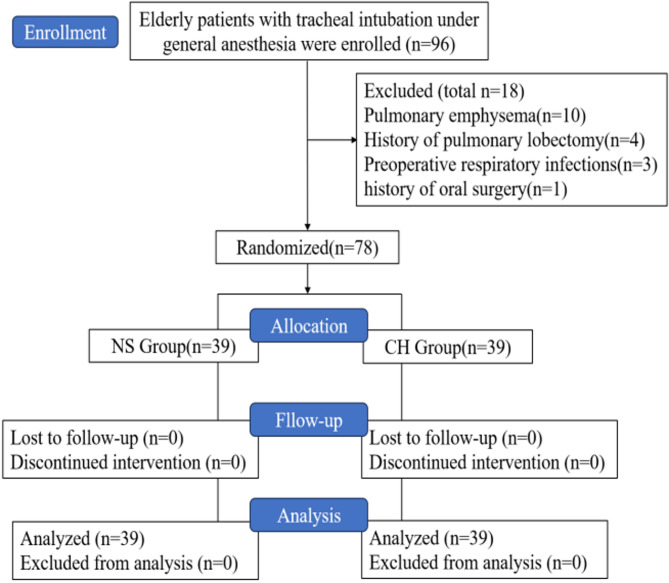
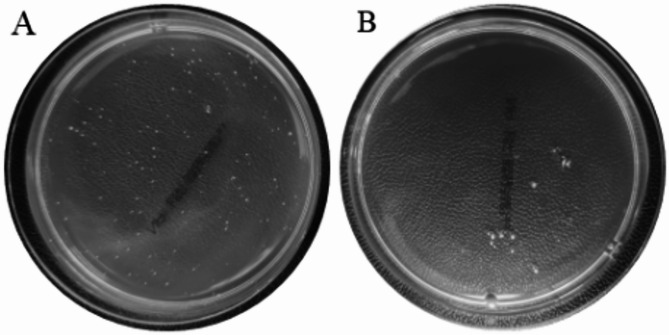
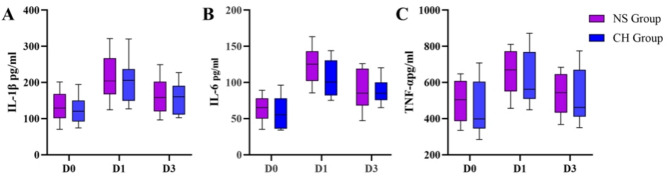
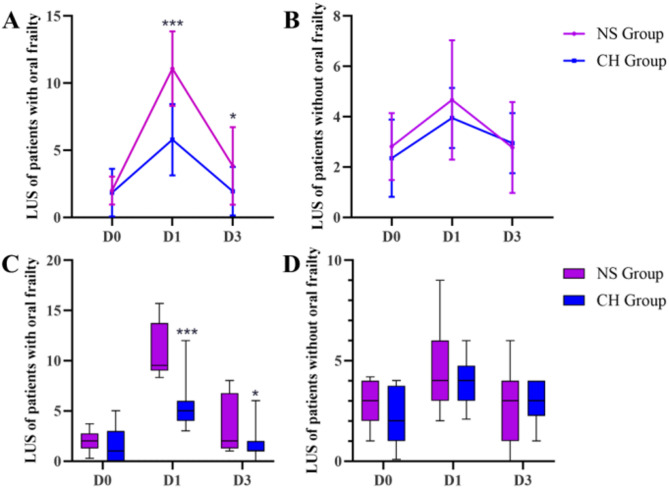
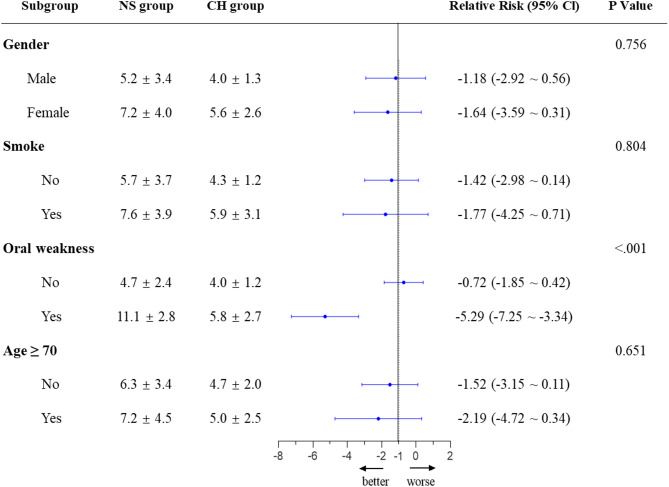
To investigate whether preoperative chlorhexidine mouthwash can reduce the risk of postoperative pulmonary complications(PPCs) in elderly patients with tracheal intubation under general anesthesia. 78 elderly patients undergoing elective surgery under general anesthesia and endotracheal intubation were randomly divided into the chlorhexidine group (CH group, n = 39) and the normal saline group (NS group, n = 39). Nurses instructed patients to gargle with 15 ml saline or compound chlorhexidine mouthwash the night before surgery, on the morning of surgery, and upon entering the operating room. The primary outcome was lung ultrasound score (LUS) on postoperative day 1 (D1). The secondary outcome was LUS on the preoperative day (D0) and postoperative day 3 (D3), bacterial colony count at the tip of the endotracheal tube, inflammatory markers (IL-1β, IL-6, TNF-α), and the incidence of postoperative fever, pneumonia, cough severity and sputum production. The CH group had significantly lower D1LUS compared to the NS group, whereas there was no significant difference in D3LUS between the groups. Within three postoperative days, there were no significant differences between the groups in cough severity, sputum production, fever, inflammatory markers, or pneumonia incidence. Bacterial colony counts on the endotracheal tube at extubation were lower in the CH group than in the NS group. Post hoc sensitivity analysis revealed that in patients with oral frailty, the number of colonies cultured at D1LUS, D3LUS, and the catheter tip in the CH group was lower than that in the NS group. However, there was no significant difference between the two groups in terms of the incidence of pneumonia and other aspects. Exploratory subgroup analysis showed that chlorhexidine mouthwash significantly reduced postoperative LUS in patients with oral frailty, while there were no significant differences in gender, smoking and age subgroups. Preoperative chlorhexidine mouthwash improved early postoperative LUS in elderly patients by reducing oropharyngeal bacterial colonization, particularly in those with oral weakness, though clinical outcomes like pneumonia showed no significant differences. Chinese clinical trial registration number: ChiCTR2400089898.
Keywords: Chlorhexidine mouthwash; Elderly; Endotracheal intubation; Lung ultrasound; Oral frailty.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures

Similar articles
-
Chewing gum on postoperative oral Malodor in patients undergoing general anesthesia: a randomized non-inferiority trial.BMC Anesthesiol. 2025 May 21;25(1):257. doi: 10.1186/s12871-025-03134-7. BMC Anesthesiol. 2025. PMID: 40399834 Free PMC article. Clinical Trial.
-
Safety and efficacy of low-dose esketamine weakly opioidized anesthesia in elderly patients with lumbar spinal stenosis undergoing surgery: a prospective, double-blind randomized controlled trial.BMC Anesthesiol. 2025 Feb 5;25(1):57. doi: 10.1186/s12871-025-02908-3. BMC Anesthesiol. 2025. PMID: 39910473 Free PMC article. Clinical Trial.
-
[Efficacy of 1% povidone-iodine mouthwash combined with scaling and root planing in the treatment of periodontitis: a randomized, controlled trial].Hua Xi Kou Qiang Yi Xue Za Zhi. 2025 Jun 1;43(3):362-369. doi: 10.7518/hxkq.2025.2024326. Hua Xi Kou Qiang Yi Xue Za Zhi. 2025. PMID: 40523816 Free PMC article. Clinical Trial. Chinese.
-
Chlorhexidine mouthrinse as an adjunctive treatment for gingival health.Cochrane Database Syst Rev. 2017 Mar 31;3(3):CD008676. doi: 10.1002/14651858.CD008676.pub2. Cochrane Database Syst Rev. 2017. PMID: 28362061 Free PMC article.
-
Preoperative blood transfusions for sickle cell disease.Cochrane Database Syst Rev. 2016 Apr 6;4(4):CD003149. doi: 10.1002/14651858.CD003149.pub3. Cochrane Database Syst Rev. 2016. Update in: Cochrane Database Syst Rev. 2020 Jul 2;7:CD003149. doi: 10.1002/14651858.CD003149.pub4. PMID: 27049331 Free PMC article. Updated.
References
-
- Sing, C. W. et al. Global epidemiology of hip fractures: secular trends in incidence rate, Post-Fracture treatment, and All-Cause mortality. J. Bone Min. Res.38, 1064–1075. 10.1002/jbmr.4821 (2023). - PubMed
-
- Kain, Z. N., Fitch, J. C., Kirsch, J. R., Mets, B. & Pearl, R. G. Future of anesthesiology is perioperative medicine: a call for action. Anesthesiology122, 1192–1195. 10.1097/ALN.0000000000000680 (2015). - PubMed
-
- Vetrugno, L. et al. Active ageing interdisciplinary, accuracy of preoperative lung ultrasound score for the prediction of major adverse cardiac events in elderly patients undergoing HIP surgery under spinal anesthesia: the LUSHIP multicenter observational prospective study. Anaesth. Crit. Care Pain Med.43, 101432. 10.1016/j.accpm.2024.101432 (2024). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
