

Incidence and predictors of extubation failure among adult intensive care unit patients in Northwest Amhara comprehensive specialized hospitals
- PMID: 40594652
- PMCID: PMC12215632
- DOI: 10.1038/s41598-025-05625-6
Incidence and predictors of extubation failure among adult intensive care unit patients in Northwest Amhara comprehensive specialized hospitals
Abstract
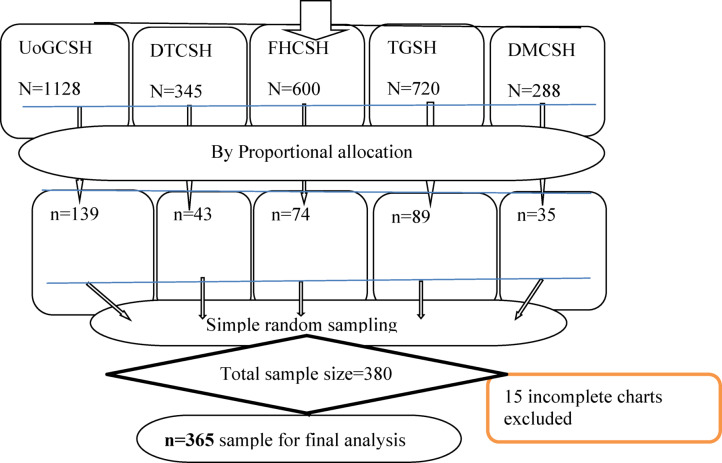
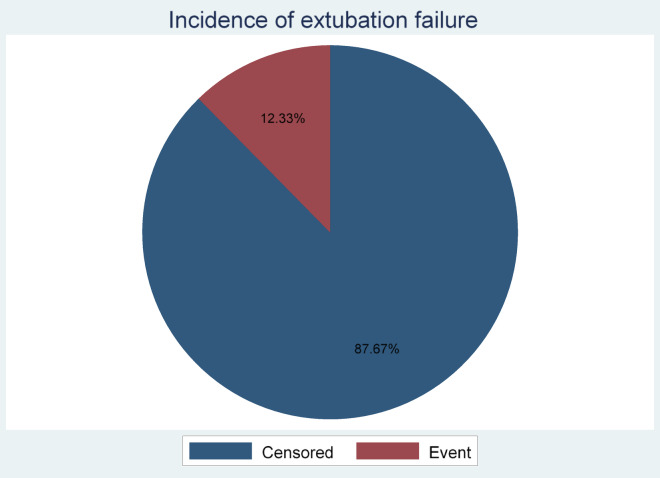
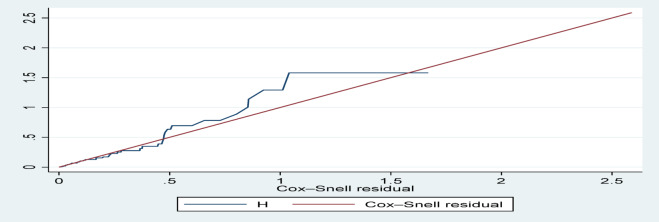
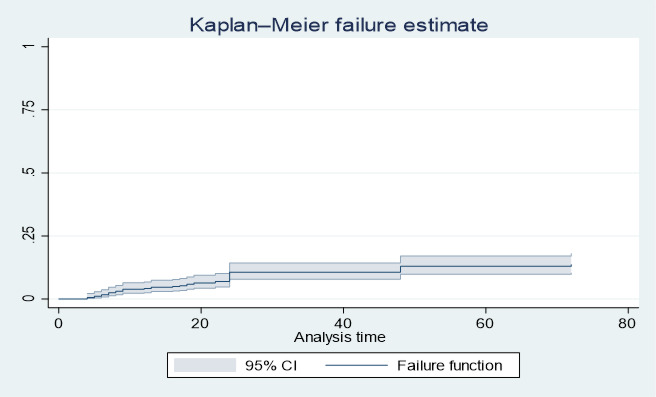
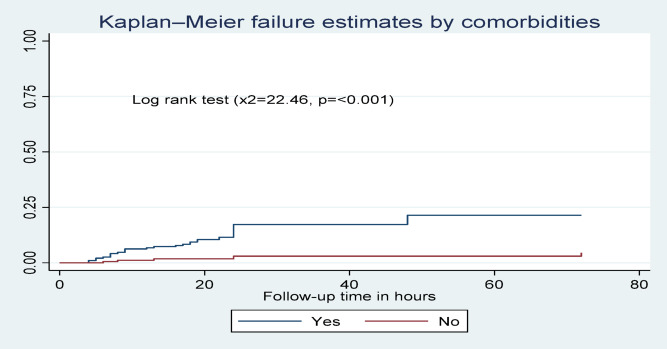
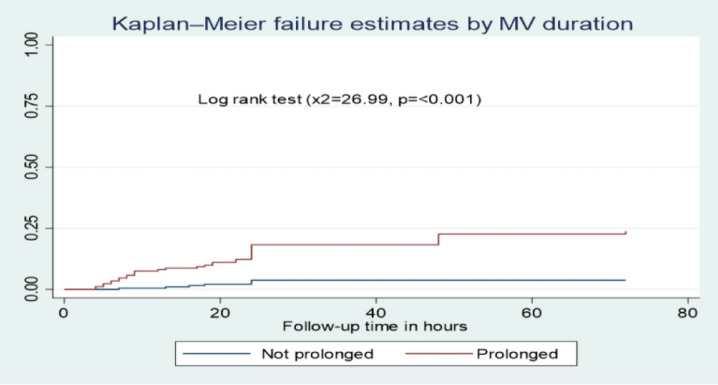
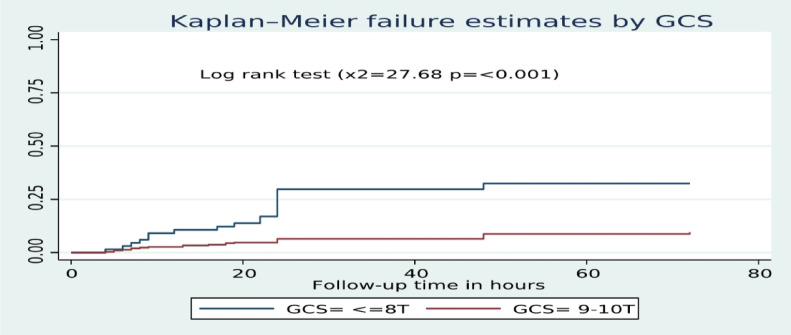
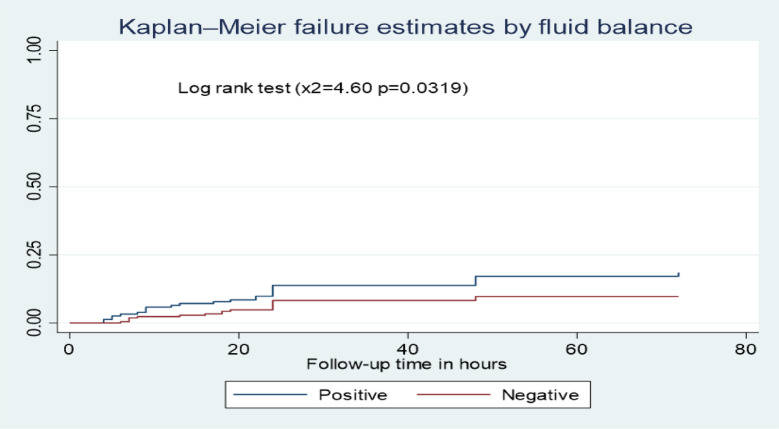
Extubation failure occurs in mechanically ventilated patients after planned extubation. It can cause increased mortality, length of intensive care unit stays, prolonged mechanical ventilation use, increased hospital costs, and increased need for tracheostomy. In Ethiopia, extubation failure is limitedly studied among adult patients admitted to intensive care units. Therefore, this study aimed to assess the incidence and predictors of extubation failure among adult patients in intensive care units. A multicenter retrospective follow-up study was conducted among 380 extubated patients from mechanical ventilation at the intensive care unit in northwest Amhara comprehensive specialized hospitals from May 1, 2021, to April 30, 2024. The data was collected randomly from patient cards using a simple random method with a pretested checklist. The data was entered using Epi-Data 4.6 and analyzed using STATA 17. The Kaplan-Meier curve was used to estimate the median extubation failure time. The Cox proportional hazard regression model analyzes the relationship between independent and outcome variables. The overall incidence of extubation failure was 2.64 (95% CI: 1.97-3.54) per 1000 person-hour observations. Forty-five (12.33%) of participants had developed extubation failure. Comorbidities (AHR: 3.92, 95% CI: 1.41-10.81), prolonged mechanical ventilation duration (AHR: 4.69, 95% CI: 2.04-10.80), GCS ≤ 8 with tracheal intubation (AHR: 4.10, 95% CI: 2.10-7.97), and positive fluid balance (AHR: 2.39, 95% CI: 1.23-4.62) were independent predictors of extubation failure. Extubation failure among adult patients admitted to the intensive care unit was high in the first 24 h after extubation. The risk of extubation failure was higher for those patients with comorbidities, prolonged mechanical ventilation, GCS ≤ 8 with tracheal intubation, and positive fluid balance. Therefore, clinicians should prioritize patients who have comorbid conditions, require extended mechanical ventilation, have a Glasgow Coma Scale score of 8 or lower with tracheal intubation, or exhibit a positive fluid balance.
Keywords: Extubation failure; Incidence; Intensive care unit; Northwest Ethiopia; Predictors.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures
References
-
- Whitmore, D. & Mahambray, T. Reintubation following planned extubation: incidence, mortality and risk factors. Intensive Care Med. Experimental. 3 (Suppl 1), A684 (2015). - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
