

Immunogenicity and safety of mRNA-based seasonal influenza vaccines encoding hemagglutinin and neuraminidase
- PMID: 40595624
- PMCID: PMC12216828
- DOI: 10.1038/s41467-025-60938-4
Immunogenicity and safety of mRNA-based seasonal influenza vaccines encoding hemagglutinin and neuraminidase
Abstract
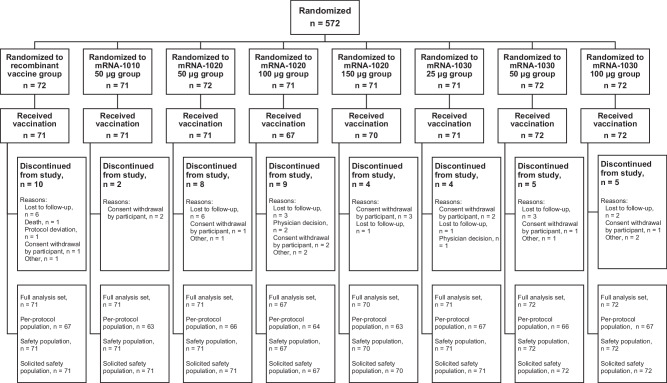
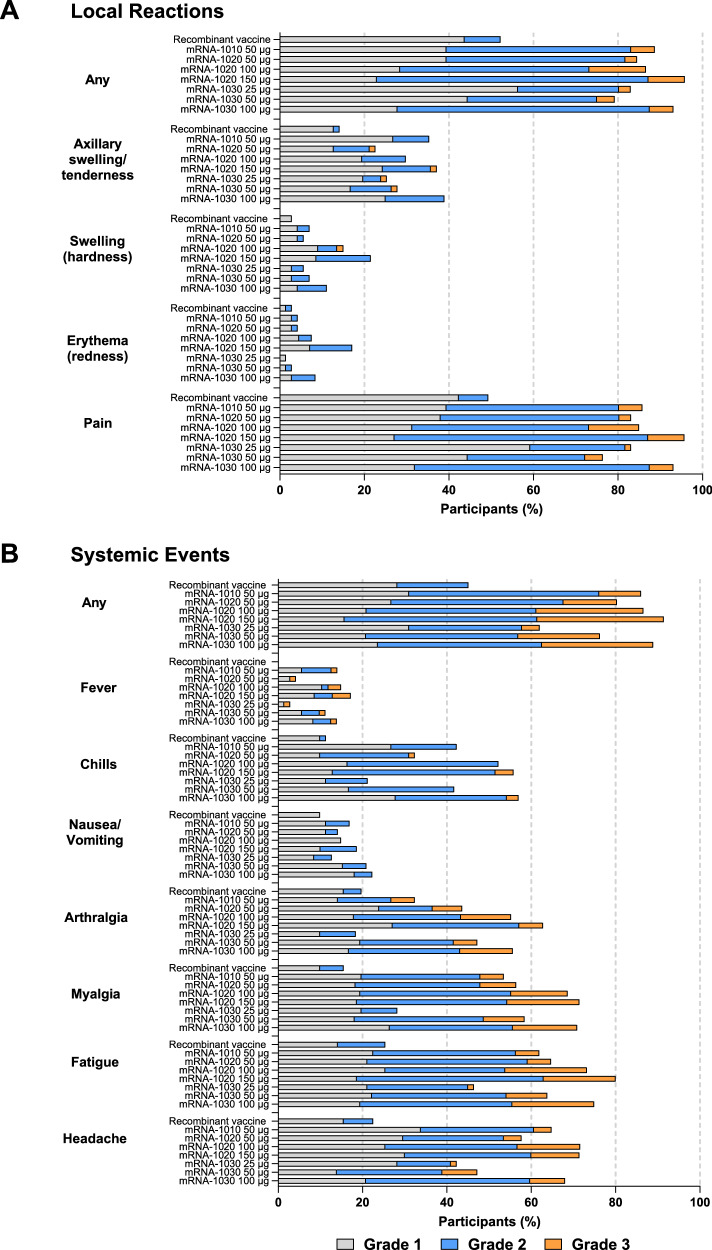
Current influenza vaccines induce immune responses to hemagglutinin (HA), a surface glycoprotein of seasonal influenza viruses, but have suboptimal effectiveness. mRNA vaccines may improve protection by targeting additional antigens such as neuraminidase (NA), for which immune responses independently correlate with protection. In this phase 1/2 trial (NCT05333289), healthy adults 18-75 years were randomly assigned to receive different doses of mRNA-1020 or mRNA-1030 (encoding HA and NA at different ratios), mRNA-1010 (encoding HA), or a licensed active comparator (recombinant HA). Primary endpoints were safety and reactogenicity, and HA and NA antibody responses against vaccine-matched influenza strains. Most common local and systemic solicited ARs were injection site pain and fatigue. There were no vaccine-related serious adverse events nor significant associated safety concerns through 181 days. mRNA-1020 and mRNA-1030 elicited high HA-specific immune responses and induced NA-specific immune responses with no additional reactogenicity at equivalent dose levels beyond an mRNA-based, HA-only-containing vaccine.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: A.K.R.S., K.K., K.S., A.A., D.S., B.H., A.P., J.V., R.P., and R.N. are employees of Moderna, Inc., and may hold stock/stock options in the company. I.T.L. and J.A. were employees of Moderna, Inc., at the time of the study. D.E., D.K.L., and J.H. declare no competing interests.
Figures



References
-
- World Health Organization. Vaccines against influenza: WHO position paper - May 2022. Wkly. Epidemiol. Rec.87, 185–208 (2022).
-
- Yamayoshi, S. & Kawaoka, Y. Current and future influenza vaccines. Nat. Med25, 212–220 (2019). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
