

Nomogram for the prediction of the prognosis of patients with triple-negative invasive ductal carcinoma of breast after neoadjuvant chemotherapy
- PMID: 40596034
- PMCID: PMC12215188
- DOI: 10.1038/s41598-025-05738-y
Nomogram for the prediction of the prognosis of patients with triple-negative invasive ductal carcinoma of breast after neoadjuvant chemotherapy
Abstract
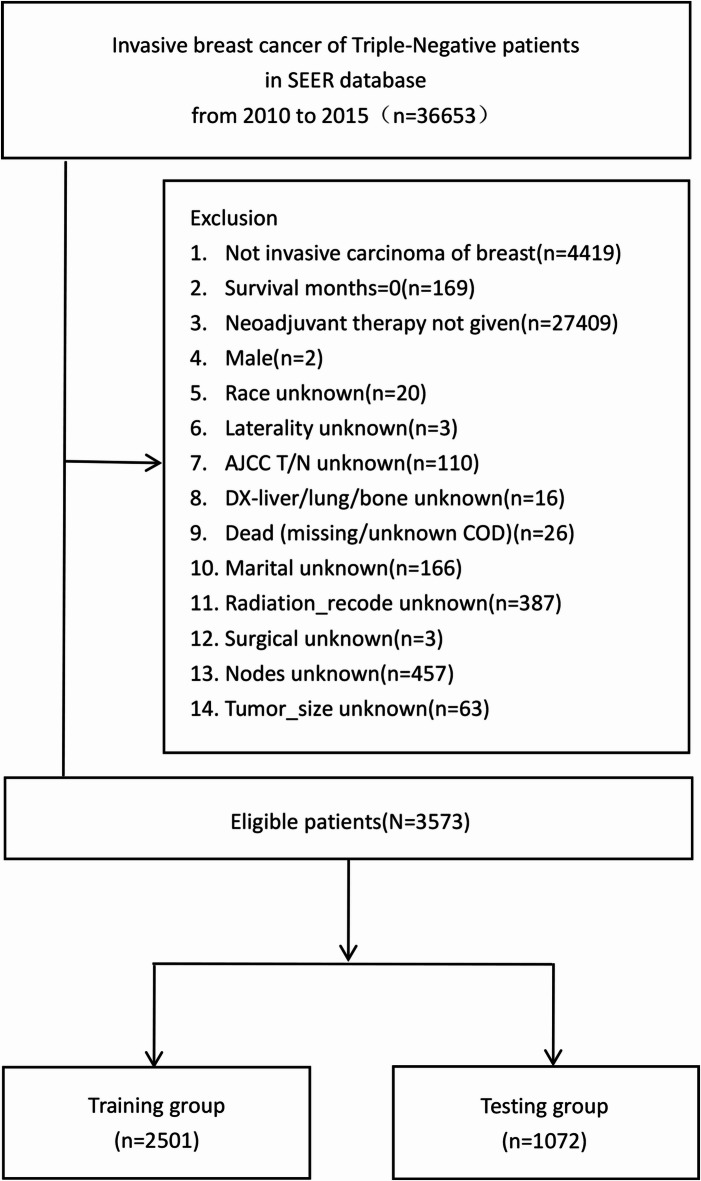
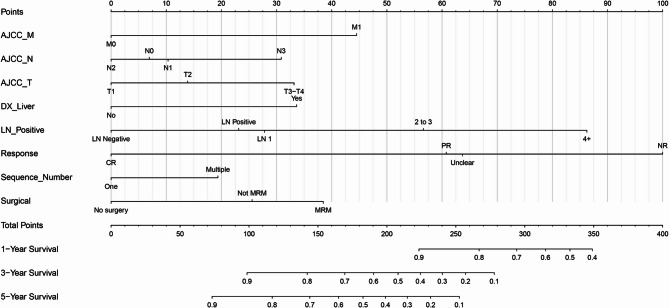
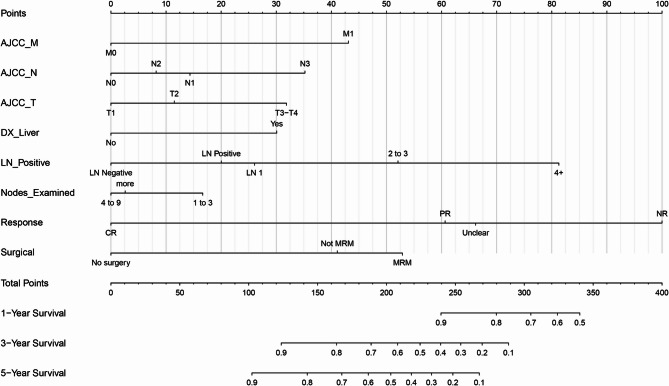
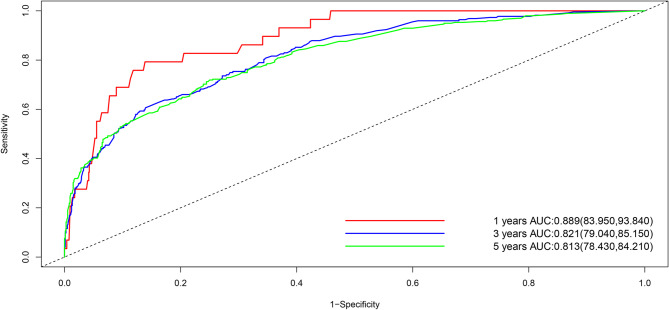
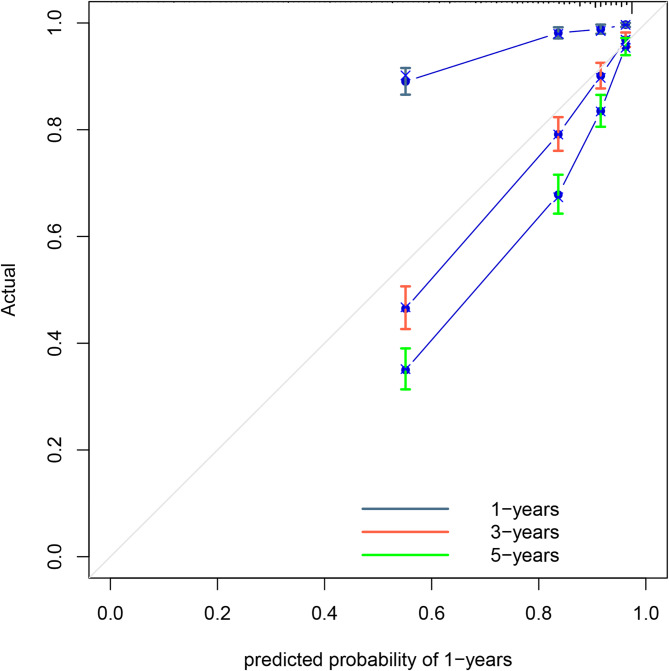
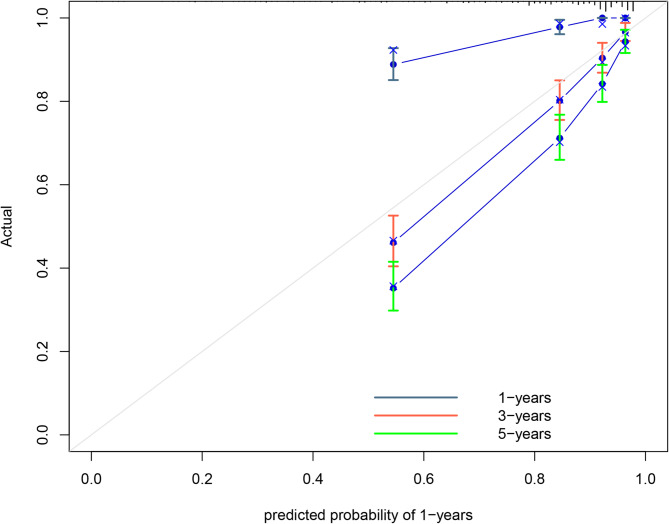
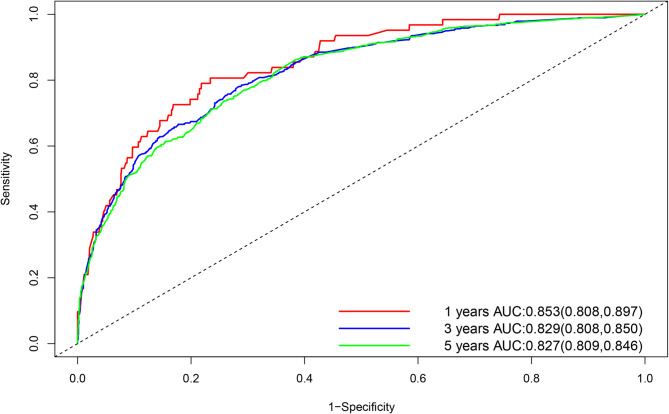
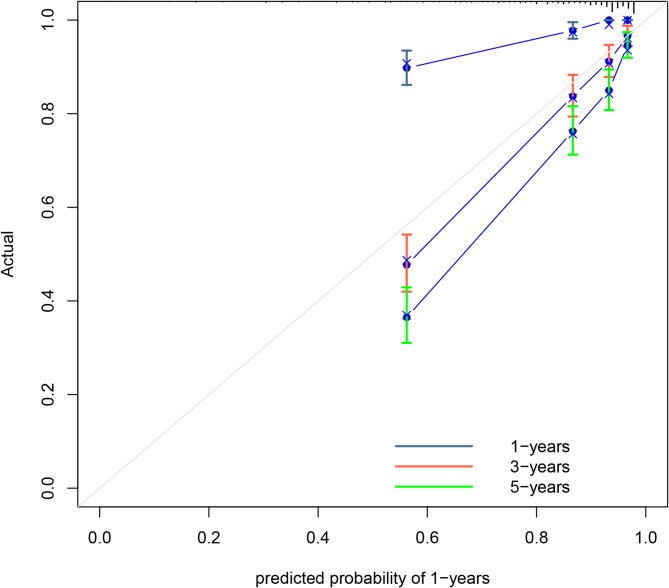
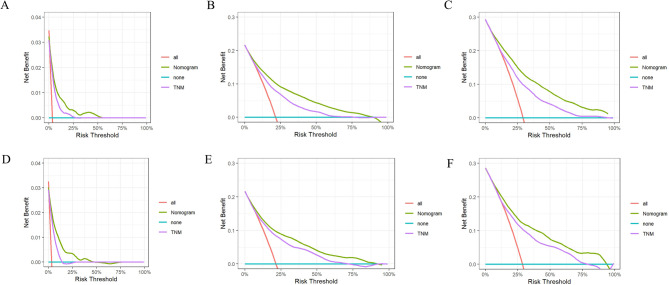
Triple-negative breast cancer (TNBC) represents a subtype of breast cancer with a poor prognosis because of limited treatment options at present. Therefore, this study aimed to use nomograms to forecast the prognosis of patients with triple-negative invasive ductal carcinoma of the breast (TN-IDC) undergoing neoadjuvant chemotherapy (NCT). 3573 TNBC patients from the SEER database who received NCT between 2010 and 2015 were selected and randomized in 7:3 into the training or the testing group. Then, nomograms for overall survival (OS) and cancer-specific survival (CSS) of the two groups were created via univariate and multivariate analyses. Consistency index (C-index), calibration curve, and area under the receiver operating characteristic curve (AUC), decision curve analysis (DCA) were employed to evaluate the reliability and accuracy of the model. As demonstrated by univariate and multivariate Cox regression analyses, 8 indicators (AJCC_M, AJCC_N, AJCC_T, positive lymph nodes [LNs] and the number of positive LNs, liver metastases, response to NCT, and radical surgery) were incorporated in the nomogram. The results indicated that the C-index of the OS prediction model was 0.776 for the training group and 0.779 for the testing group. In the training group, the AUC for forecasting 1-, 3-, and 5-year OS was 0.840, 0.822, and 0.817, respectively; in the testing group, the AUC was 0.889, 0.821, and 0.813, respectively. The C-index of the CSS prediction model was 0.790 for the training group and 0.789 for the testing group. In the training group, the AUC for forecasting 1-, 3-, and 5-year CSS was 0.853, 0.829, and 0.827, respectively; in the testing group, the AUC was 0.887, 0.800, and 0.820, respectively. Both C-index and AUC of OS and CSS prediction models were above or close to 0.8, indicating good predictability of the model. DCA consistently indicated that using the nomogram for OS and CSS prediction yielded favorable net clinical benefit, and the nomogram outperformed the AJCC TNM staging system in decision-making. T2-4 (maximum tumor diameter > 2 cm or invasion of the chest wall/skin), N3, M1, liver metastasis, incomplete remission after chemotherapy, and breast-conserving surgery were prognostic risk factors in TN-IDC patients receiving NCT. Higher T stage (T3-4, maximum tumor diameter > 5 cm or invasion of the chest wall/skin), N stage (N3), liver metastasis, non-remission (NR) after NCT, and positive LNs after chemotherapy were linked to worse OS and CSS. After NCT, the number of positive LNs ≥ 4 and NR for lesion exhibited the greatest impact on OS and CSS.
Keywords: Invasive ductal carcinoma of breast; Neoadjuvant chemotherapy; Nomogram; SEER; Triple-negative breast cancer.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures




References
-
- Borri, F. & Granaglia, A. Pathology of triple negative breast cancer. Semin. Cancer Biol.72, 136–145. 10.1016/j.semcancer.2020.06.005 (2021). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
