

Clinical efficacy and biomechanical analysis of robotic internal fixation with percutaneous screws in the treatment of both-column acetabular fractures
- PMID: 40596294
- PMCID: PMC12216115
- DOI: 10.1038/s41598-025-06168-6
Clinical efficacy and biomechanical analysis of robotic internal fixation with percutaneous screws in the treatment of both-column acetabular fractures
Abstract
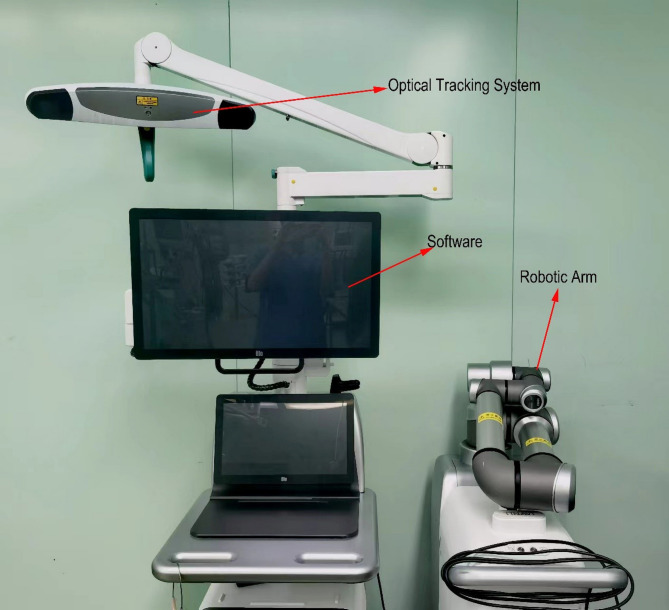
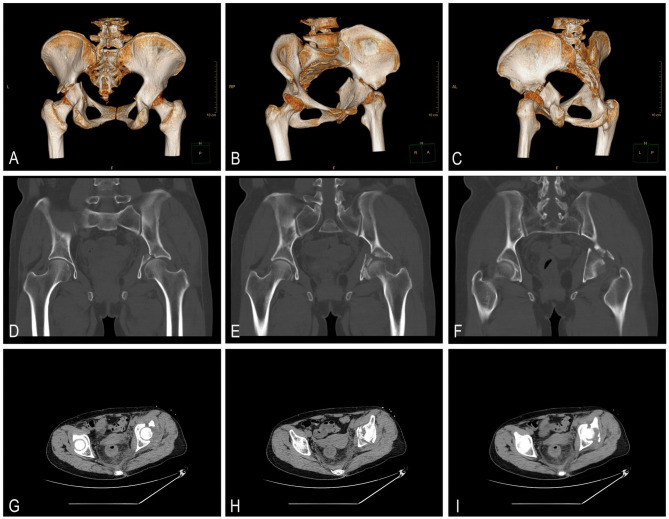
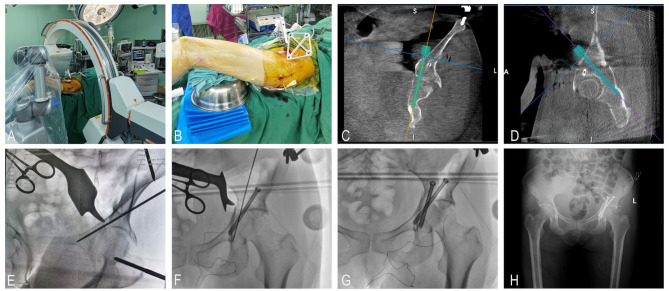
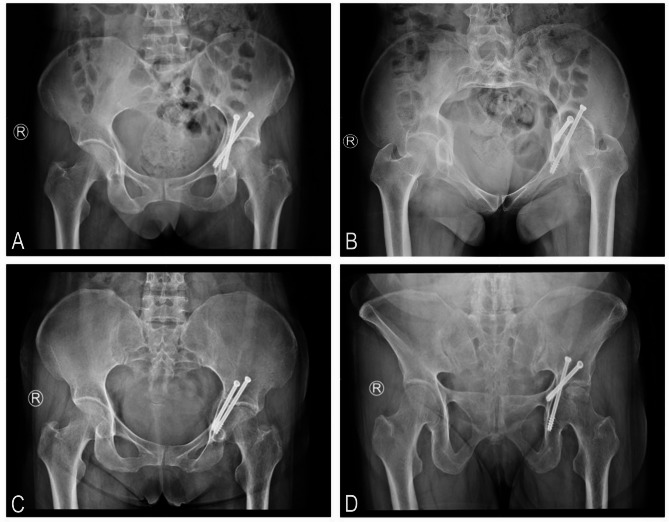
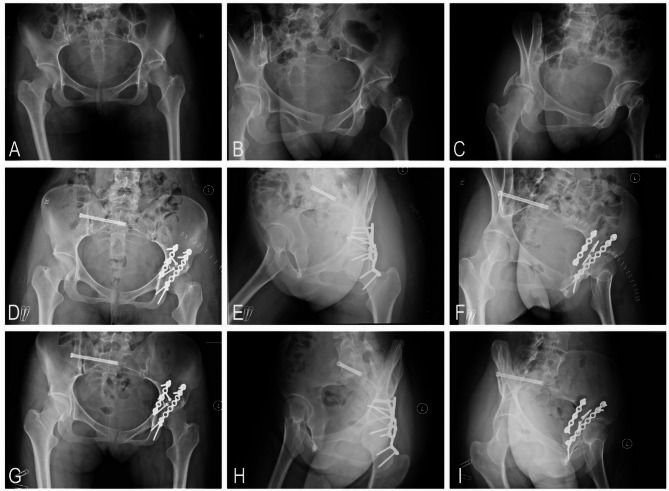
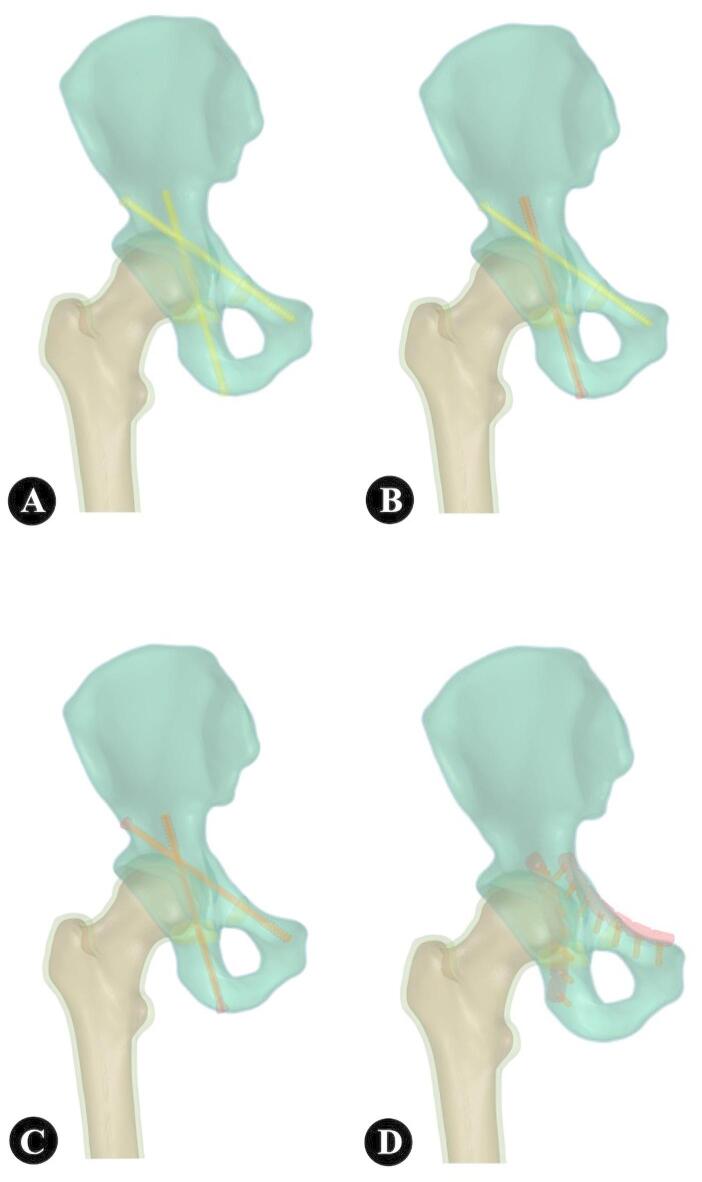
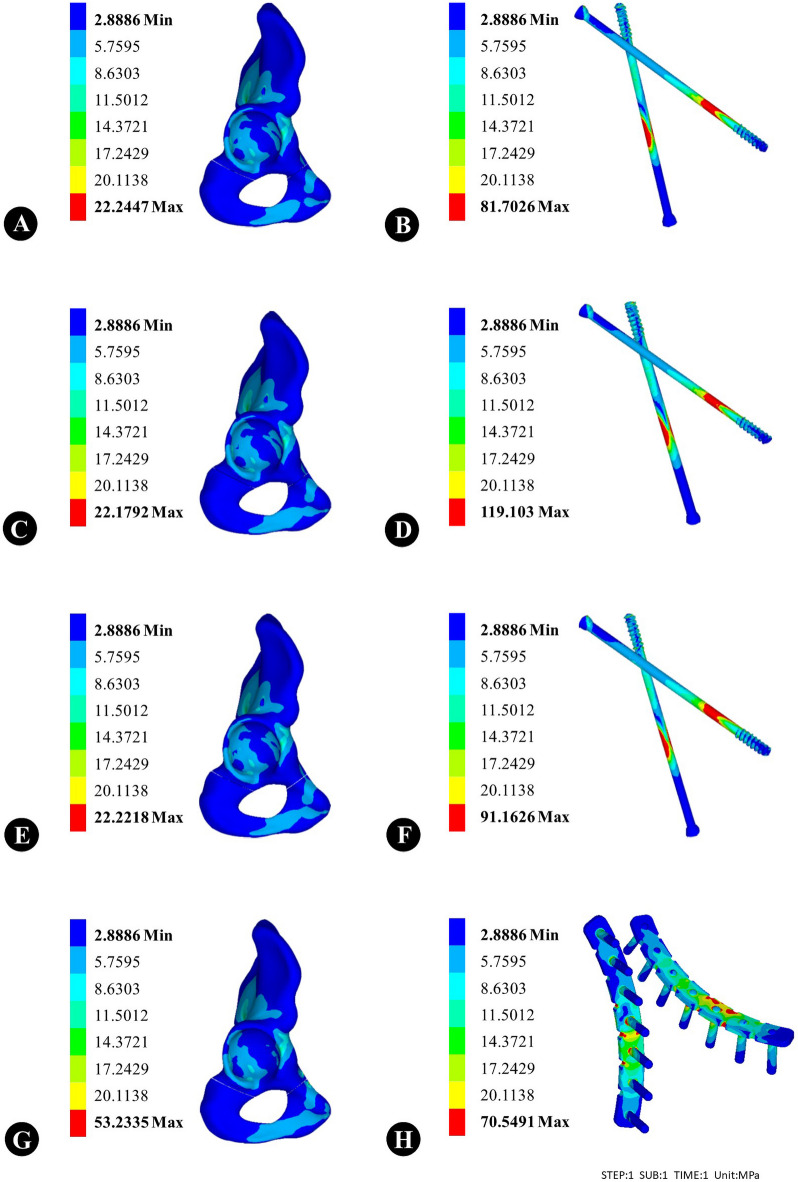
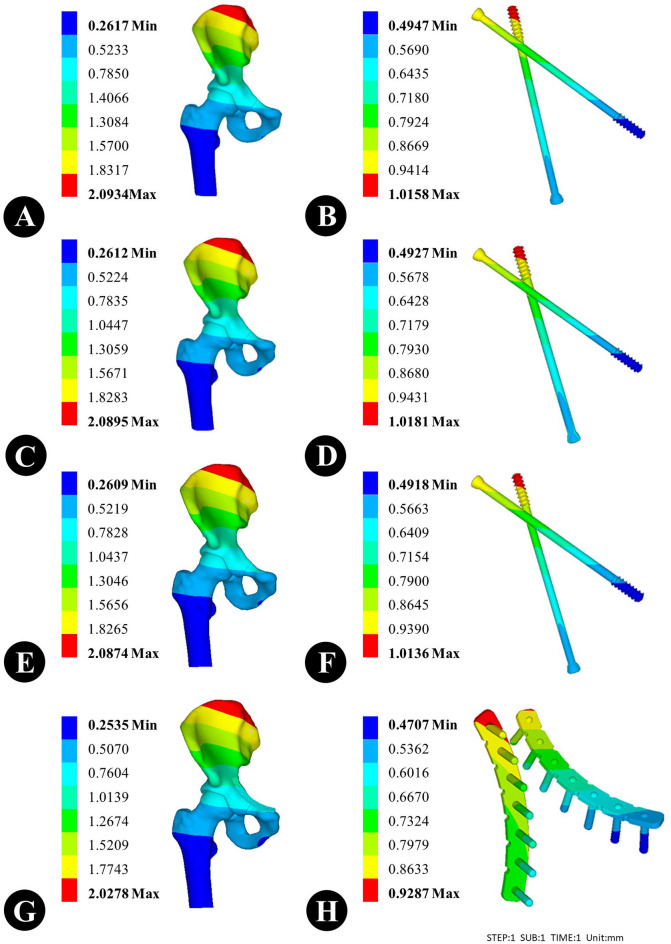
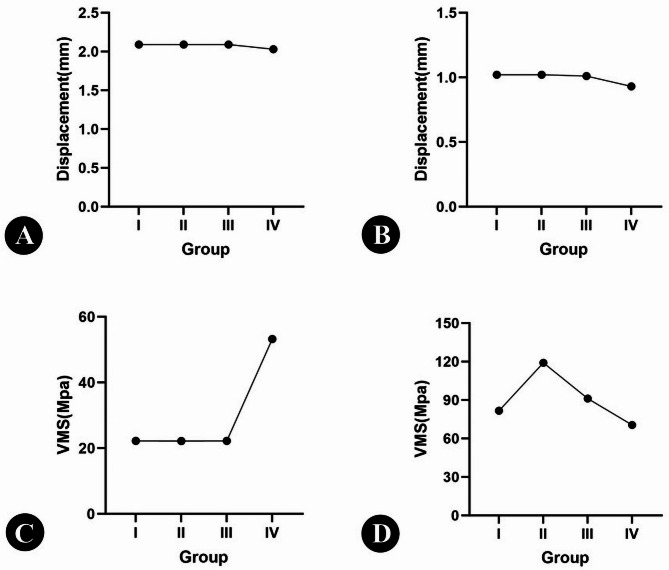
Both-column fractures of the acetabulum represent a particularly complex category of injury, with a high proportion necessitating surgical intervention. The most common surgical method is open reduction and internal fixation (ORIF), but this has problems like blood loss, long operations, and trauma after surgery. Robot-assisted percutaneous screw fixation is a minimally invasive treatment for both-column acetabular fractures. It has several clinical advantages, including precise screw positioning and stable performance. A comparison of the clinical efficacy of open reduction and internal fixation and robot-assisted percutaneous screws in the treatment of both-column acetabular fractures and biomechanical analyses were performed to compare the stability of the two fixation methods. Firstly, A finite element model was constructed for the purposes of analyzing both-column acetabular fractures, percutaneous screws, and reconstruction plates. Divided into four experimental groups: Group I: Acetabular anterior and posterior columns are screwed with a 6.5 mm percutaneous screw. Group II: The anterior column of the acetabulum is fixed with a 6.5 mm percutaneous screw, while the posterior column is fixed with a 7.3 mm percutaneous screw. Group III: Acetabular anterior and posterior columns are screwed with a 7.3 mm percutaneous screw. Group IV: Acetabular anterior and posterior columns are fixed with a 6-hole reconstruction plate. Each fracture group was tested under axial loads of 600 N to measure the hipbone's displacement, Von Mises stress (VMS), and its internal fixation components. Secondly, 36 patients with both-column acetabular fractures admitted from September 2020 to September 2023 were retrospectively analyzed; 19 of them in the ORIF group, and 17 of them in the robot-assisted group. A comparison of the operative time, duration of intraoperative fluoroscopy, intraoperative blood loss, incision length, Matta's radiological criteria, and Harris Hip Score (HHS) in two groups of patients. In terms of finite element analysis, the maximum VMS was observed for internal fixation in group II, and the minimum VMS was observed in group IV. The displacements of groups I, II, and III internal fixation were the same (approximately 1.00 mm), and the minimum internal fixation displacement was observed in group IV. The mean operating time in the ORIF group was 190.45 ± 25.40 min, the incision length was 20.56 ± 3.38 centimeters, the intraoperative bleeding was 958.73 ± 128.68 ml, and the fluoroscopy time was 55.18 ± 10.25 s. The mean operating time in the robotic group was 99.7 ± 18.8 min, with an incision length of 7.35 ± 0.56 cm, intraoperative bleeding of 50.00 ± 15.20 ml, and fluoroscopy time of 22.52 ± 14.50 s. There was a significant difference between the above data (P < 0.001). There was no significant difference in Matta's radiological criteria between the two groups. HHS at three months postoperatively and six months postoperatively were 77.81 ± 2.23 and 84.78 ± 4.65 in the ORIF group, and at three months postoperatively and six months postoperatively in the robotic group were 72.19 ± 1.85 and 82.28 ± 3.32. The use of robot-assisted percutaneous screw internal fixation for both-column acetabular fractures has been demonstrated to have similar fixed strength and therapeutic effect to that of ORIF plate fixation. In contrast, robot-assisted percutaneous screw therapy offers the advantages of minimal invasiveness and precision, thereby providing a novel therapeutic option for the clinical treatment of both-column acetabular fractures.
Keywords: Both-column acetabular fractures; Finite element analysis; Percutaneous screw.; Robot.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
The Kocher-Langenbeck approach combined with TiRobot-assisted percutaneous anterior column screw fixation for transverse with or without posterior wall fractures of acetabulum: a retrospective study.Int Orthop. 2025 Aug;49(8):1989-1999. doi: 10.1007/s00264-025-06571-8. Epub 2025 Jun 20. Int Orthop. 2025. PMID: 40540034
-
[Analysis of effectiveness of Holosight robot navigation-assisted percutaneous cannulated screw fixation in treatment of femoral neck fractures].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2025 Jun 15;39(6):673-679. doi: 10.7507/1002-1892.202502067. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2025. PMID: 40545454 Free PMC article. Chinese.
-
Mg-Zn-Ca Alloy (ZX00) Screws Are Resorbed at a Mean of 2.5 Years After Medial Malleolar Fracture Fixation: Follow-up of a First-in-humans Application and Insights From a Sheep Model.Clin Orthop Relat Res. 2024 Jan 1;482(1):184-197. doi: 10.1097/CORR.0000000000002799. Epub 2023 Aug 21. Clin Orthop Relat Res. 2024. PMID: 37603369 Free PMC article.
-
Surgical interventions for treating intracapsular hip fractures in older adults: a network meta-analysis.Cochrane Database Syst Rev. 2022 Feb 14;2(2):CD013404. doi: 10.1002/14651858.CD013404.pub2. Cochrane Database Syst Rev. 2022. PMID: 35156192 Free PMC article.
-
Surgical versus non-surgical interventions for displaced intra-articular calcaneal fractures.Cochrane Database Syst Rev. 2023 Nov 7;11(11):CD008628. doi: 10.1002/14651858.CD008628.pub3. Cochrane Database Syst Rev. 2023. PMID: 37933733 Free PMC article.
References
-
- Banaszek, D., Starr, A. J. & Lefaivre, K. A. Technical considerations and fluoroscopy in percutaneous fixation of the pelvis and acetabulum. J. Am. Acad. Orthop. Surg.27 (24), 899–908 (2019). - PubMed
-
- Boudissa, M. et al. Epidemiology and treatment of acetabular fractures in a level-1 trauma centre: Retrospective study of 414 patients over 10 years. Orthop. Traumatol. Surg. Res.103 (3), 335–339 (2017). - PubMed
-
- Bulaqi, H. A. et al. Dynamic nature of abutment screw retightening: Finite element study of the effect of retightening on the settling effect. J. Prosthet. Dent.113 (5), 412–419 (2015). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
