

Urinary NephroCheck® test, as a marker of subclinical postoperative AKI, correlates with long-term GFR decline in patients undergoing partial nephrectomy: a prospective bicentric observational study
- PMID: 40596929
- PMCID: PMC12220470
- DOI: 10.1186/s12882-025-04242-9
Urinary NephroCheck® test, as a marker of subclinical postoperative AKI, correlates with long-term GFR decline in patients undergoing partial nephrectomy: a prospective bicentric observational study
Abstract
Background: Nephron-sparing surgery (NSS) represents the preferred technique to treat localized renal lesions, not being exempted from the risk of postoperative acute kidney injury (AKI) to happen, though. Patients experiencing postoperative AKI, either clinical or subclinical, are more susceptible to develop chronic kidney disease.
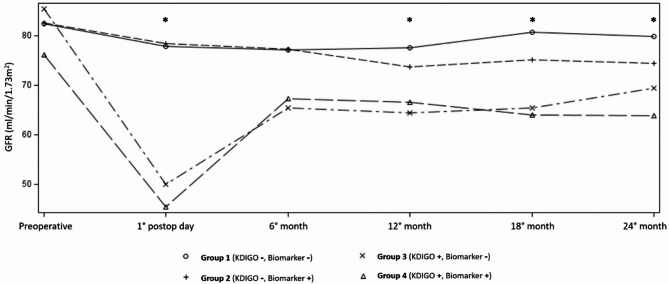
Methods: Patients scheduled for NSS in localized renal cell carcinoma were recruited. Patients were grouped according to postoperative AKI development and postoperative NephroCheck value: group 1 (normal), no AKI and no increased biomarker; group 2 (subclinical AKI), no AKI but increased NephroCheck (> 0.3 at 4 h postoperatively); group 3, AKI and no increased NephroCheck; group 4 (clinical AKI), AKI and increased NephroCheck. Samples were collected pre- and post-operatively; renal function was re-assessed up to 24 months.
Results: Among 131 patients included, 42% developed clinical AKI. Based on NephroCheck® and clinical AKI criteria, patients could be divided in four groups with significantly different eGFR at 24 months (p = 0.0003). Multivariate analysis confirmed clinical AKI as an independent predictor of eGFR decline at 24 months (p < 0.0003). In subclinical AKI's subgroup [20/131 (15%)], characterized by urinary NephroCheck® >0.3 and serum creatinine increase < 0.3 mg/dL, NephroCheck® appeared as an independent predictor of severe eGFR decline at 24 months (OR 3.76, p = 0.02); in this subgroup, eGFR decline resulted significantly more severe compared to eGFR decline in patients with neither serum creatinine nor tubular damage markers' elevation.
Conclusions: In patients undergoing NSS, the most reliable predictor of long-term eGFR decline is represented by the occurrence of postoperative clinical AKI. In this setting, NephroCheck® appeared able to identify 'subclinical AKI' and consequently patients at increased risk of 24-month-eGFR decline.
Keywords: Acute kidney injury; IGFBP7; NephroCheck; Partial nephrectomy; Renal cell carcinoma; TIMP-2.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: Informed written consent to participate was obtained from all of the participants in the study. The study was conducted in accordance with the Declaration of Helsinki; the study protocol was approved by local ethics committees (Comitato Etico Regionale per la Sperimentazione Clinica della Regione Toscana, study approval number BIO.16.015, and University of Heidelberg’s Ethics Committee II, Medical Faculty Mannheim, study approval number 2015-549N). Clinical trial number: not applicable. Consent for publication: Informed written consent was obtained from all subjects involved in the study. There are no identifying images or other personal or clinical details of participants that could compromise anonymity. Competing interests: The authors declare no competing interests.
Figures


References
-
- Wu J, Suk-Ouichai C, Dong W, et al. Analysis of survival for patients with chronic kidney disease primarily related to renal cancer surgery. BJU Int. 2018;121(1):93–100. 10.1111/bju.13994. - PubMed
-
- Schmid M, Krishna N, Ravi P, et al. Trends of acute kidney injury after radical or partial nephrectomy for renal cell carcinoma. Urol Oncol. 2016;34(7):293e. 1-293.e10. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
