

Diagnostic performances of adding transition and hepatobiliary phase to washout in gadoxetic acid-enhanced MRI for subcentimeter hepatocellular carcinoma
- PMID: 40596938
- PMCID: PMC12211149
- DOI: 10.1186/s12876-025-04071-y
Diagnostic performances of adding transition and hepatobiliary phase to washout in gadoxetic acid-enhanced MRI for subcentimeter hepatocellular carcinoma
Abstract
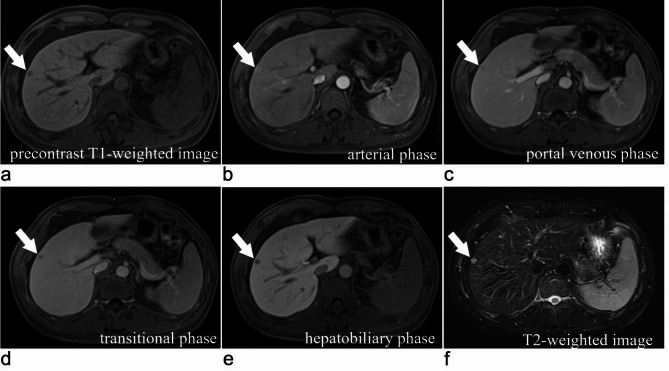
Objective: To compare the diagnostic performances of washout (WO) criteria confined to portal venous phase (PVP), extended to transition phase (TP) or hepatobiliary phase (HBP) for subcentimeter hepatocellular carcinoma (HCC) using gadoxetic acid-enhanced MRI.
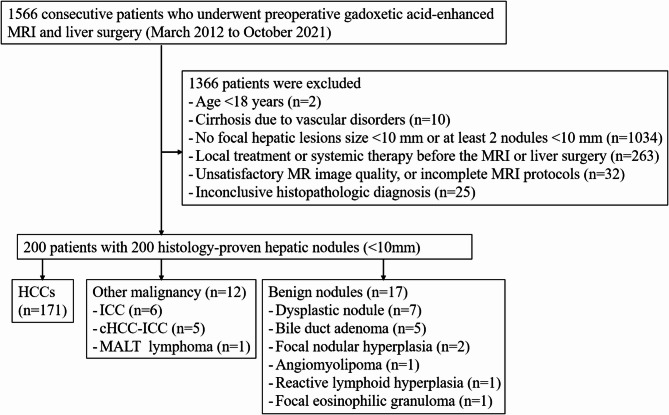
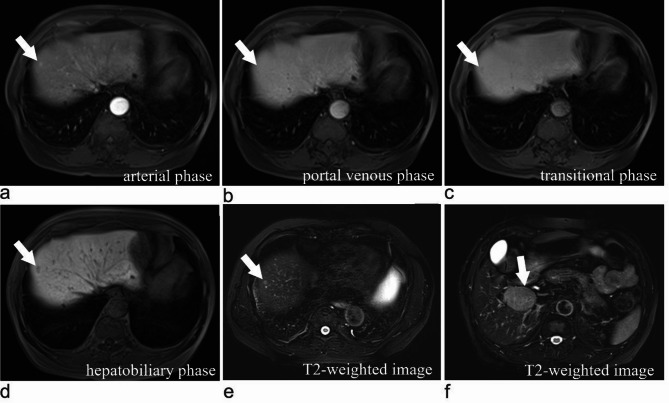
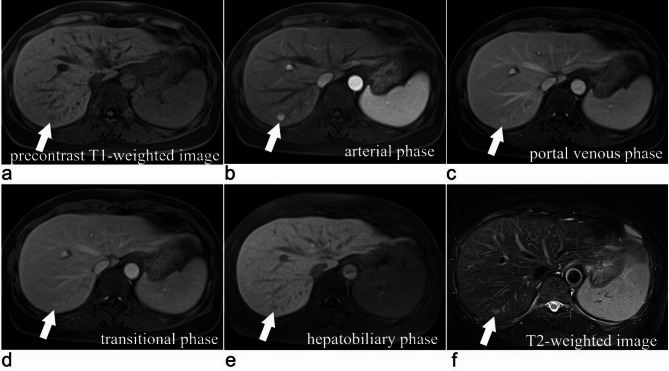
Materials and methods: Two hundred patients (mean age, 53.4 ± 10.4 years) who were scanned with 1.5-T gadoxetic acid-enhanced MRI were included. Arterial phase hyperenhancement and signal intensity on PVP, TP and HBP images were evaluated. Three WO criteria were established: WO confined to the PVP, WO extended to the TP and WO extended to the HBP.
Assessment: Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy with 95% confidence interval were calculated for WO confined to the PVP and WO extended to the TP or HBP, and generalized estimating equation was used to compare sensitivity, specificity, PPV, NPV and accuracy.
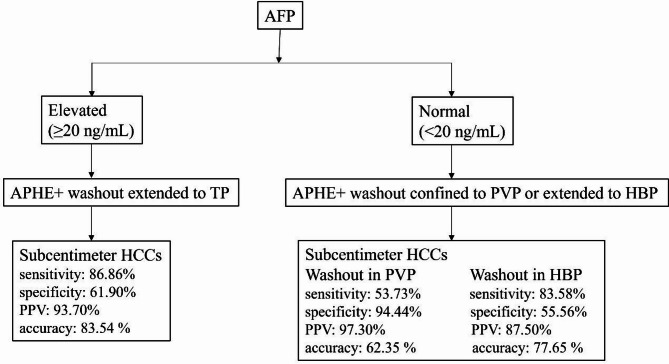
Results: A total of 200 surgically confirmed subcentimeter hepatic nodules (171 HCCs and 29 non-HCCs) were included. For solitary subcentimeter HCCs, WO extended to the TP showed significantly higher sensitivity and accuracy than WO confined to the PVP (70.80% vs. 49.64%, P < 0.05; 71.52% vs. 55.70%, P < 0.001) and AFP (70.80% vs. 51.09%, P < 0.05; 71.52% vs. 55.70%, P < 0.05), but no significant difference in specificity (76.19% vs. 95.24%, P > 0.05; 76.19% vs. 85.71%, P > 0.05). Extending WO to the HBP achieved significantly higher sensitivity (78.10% vs. 49.64%, P < 0.001; 78.10% vs. 70.80%, P < 0.05) and accuracy (75.32% vs. 55.70%, P < 0.001; 75.32% vs. 71.52%, P < 0.05) compared to WO confined to the PVP and WO extended to the TP, but lower specificity (57.14%% vs. 95.24%, P < 0.05) compared to WO confined to the PVP. The combination of AFP with WO confined to the PVP, WO extended to the TP, or WO extended to the HBP yielded significantly higher sensitivities and accuracies compared to each MRI washout criterion alone (all P < 0.001).
Conclusion: WO extending to TP rather than HBP may be a preferred alternative for diagnosing subcentimeter HCC, and the supplement of AFP may improve sensitivity and accuracy.
Keywords: Gadoxetic acid; Hepatobiliary phase; Hepatocellular carcinoma; Magnetic resonance imaging; Subcentimeter; Transition phase.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This single-center retrospective study was approved by Zhongshan Hospital of Fudan University Ethics Committee (No. B2020-372R) and the committee agreed that the requirement for patient written informed consent was waived. All methods were conducted in accordance with the principles outlined in the 1964 Declaration of Helsinki and its later amendments. Consent for publication: Not applicable. Human Ethics and Consent to Participate: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
An improved diagnostic algorithm for subcentimeter hepatocellular carcinoma on gadoxetic acid-enhanced MRI.Eur Radiol. 2023 Apr;33(4):2735-2745. doi: 10.1007/s00330-022-09282-5. Epub 2022 Dec 6. Eur Radiol. 2023. PMID: 36472696
-
Do transition and hepatobiliary phase hypointensity improve LI-RADS categorization as an alternative washout: a systematic review and meta-analysis.Eur Radiol. 2022 Aug;32(8):5134-5143. doi: 10.1007/s00330-022-08665-y. Epub 2022 Mar 10. Eur Radiol. 2022. PMID: 35267090
-
Hepatobiliary-Phase Hypointense Nodules Without Arterial-Phase Hyperenhancement: Developing a Risk Stratification for Hypervascular Transformation Based on a Real-World Observational Cohort Study.Technol Cancer Res Treat. 2024 Jan-Dec;23:15330338241299003. doi: 10.1177/15330338241299003. Technol Cancer Res Treat. 2024. PMID: 39544080 Free PMC article.
-
Interactive Explainable Deep Learning Model for Hepatocellular Carcinoma Diagnosis at Gadoxetic Acid-enhanced MRI: A Retrospective, Multicenter, Diagnostic Study.Radiol Imaging Cancer. 2025 May;7(3):e240332. doi: 10.1148/rycan.240332. Radiol Imaging Cancer. 2025. PMID: 40445095 Free PMC article.
-
Hepatic Adenoma Subtypes on Hepatobiliary Phase of Gadoxetic Acid-Enhanced MRI: Systematic Review and Meta-Analysis.AJR Am J Roentgenol. 2023 Jan;220(1):28-38. doi: 10.2214/AJR.22.27989. Epub 2022 Aug 3. AJR Am J Roentgenol. 2023. PMID: 35920706 Free PMC article.
References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Cancer J Clin. 2021;71:209–49. - PubMed
-
- Goutte N, Sogni P, Bendersky N, Barbare JC, Falissard B, Farges O. Geographical variations in incidence, management and survival of hepatocellular carcinoma in a Western country. J Hepatol. 2017;66:537–44. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- Grant No. 82202112/Youth Project of National Natural Science Foundation of China
- Grant No. 2023J05293/Youth Project of Natural Science Foundation of Fujian Province
- Grant No. 20204Y0346/Youth Foundation of Shanghai Municipal Health Commission
- Grant No. SHDC2020CR1029B/Clinical Research Plan of SHDC
- Grant No. 82171897/National Natural Science Foundation of China
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
