

The effects of remimazolam and propofol on delirium following anesthesia and sedation in elderly patients: a systematic review and meta-analysis
- PMID: 40597651
- PMCID: PMC12211366
- DOI: 10.1186/s12871-025-03167-y
The effects of remimazolam and propofol on delirium following anesthesia and sedation in elderly patients: a systematic review and meta-analysis
Abstract
Background: Delirium is a prevalent and serious postoperative complication in elderly patients, with an incidence reaching up to 70%, particularly in intensive care settings. It is associated with prolonged recovery, increased healthcare costs, and heightened mortality risk. While multifactorial etiologies involving neurotransmitter dysregulation and inflammatory cascades underline its pathogenesis, anesthetic agent selection has emerged as a modifiable risk factor requiring rigorous evaluation.
Objective: This meta-analysis aims to compare the effects of remimazolam and propofol on the incidence of delirium in elderly patients.
Methods: A systematic literature search was conducted across PubMed, Embase, the Cochrane Library, and Web of Science. Eight studies comparing remimazolam and propofol were included, encompassing a total of 1,641 patients aged ≥ 65 years patients. The primary outcome was the incidence of delirium. Secondary outcomes included the incidence of hypotension, hypoxemia, sleep disturbances, postoperative nausea and vomiting, extubation time, postoperative pain scores, and length of hospital stay.
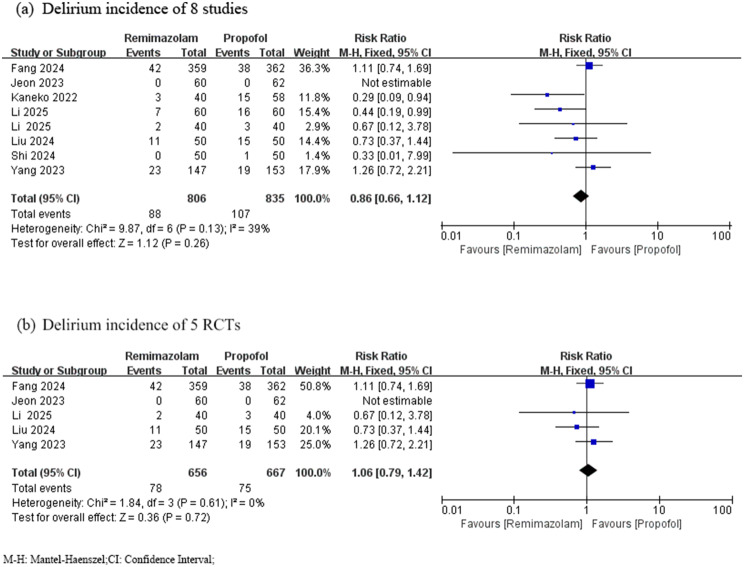
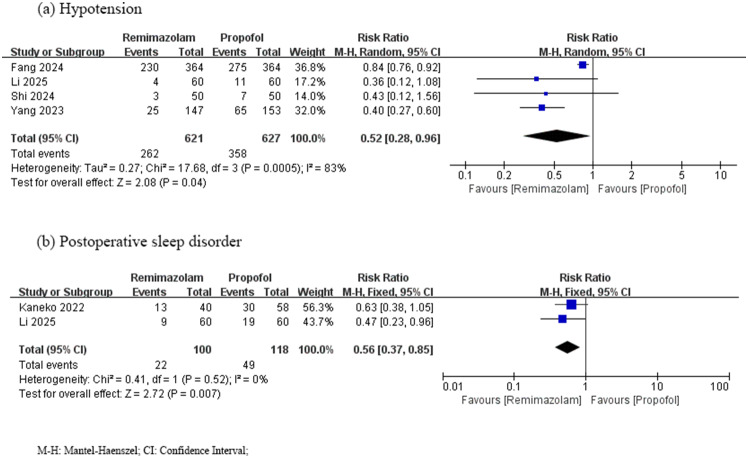
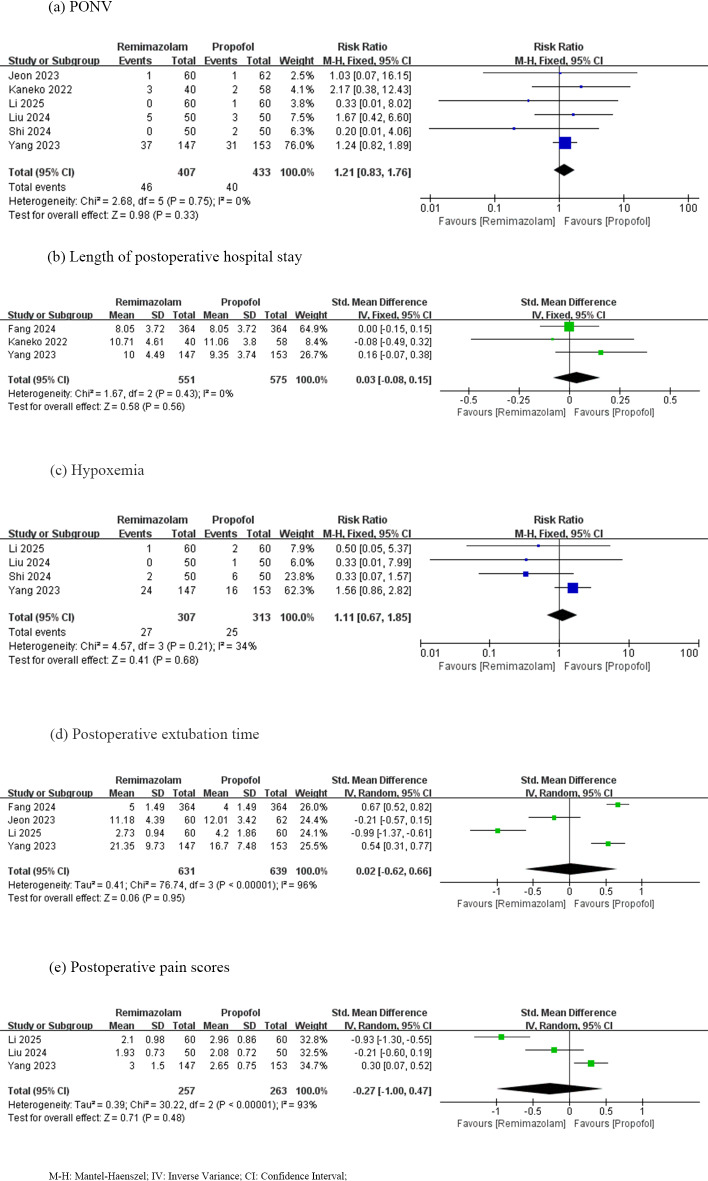
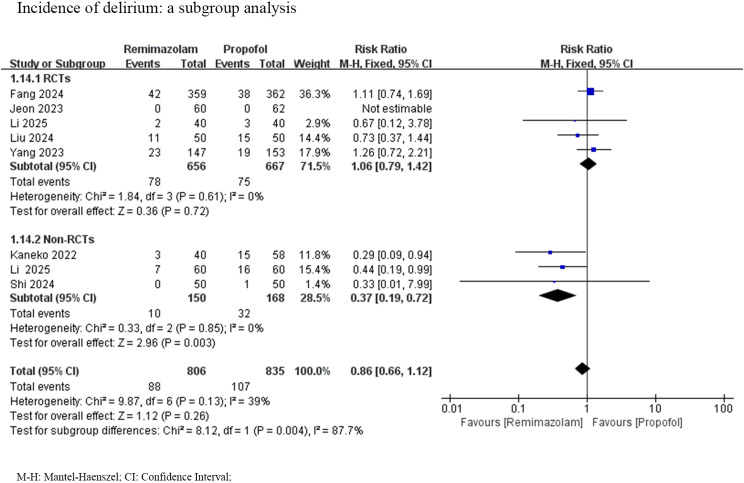
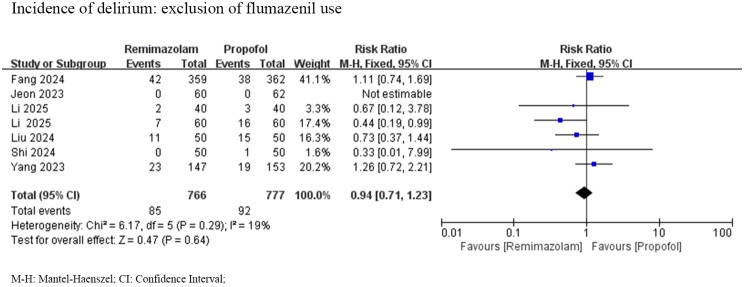
Results: The pooled analysis revealed no significant difference in delirium incidence between the remimazolam and propofol groups [relative risk (RR) = 0.86, 95% confidence interval (CI): 0.66–1.12, P = 0.26, I² = 39%]. However, remimazolam was associated with a significantly lower incidence of hypotension (RR = 0.52, 95% CI: 0.28–0.96, P = 0.04) and sleep disturbances (RR = 0.56, 95% CI: 0.37–0.85, P = 0.007) compared to propofol. No significant differences were observed in other secondary outcomes.
Conclusion: This meta-analysis suggests that remimazolam and propofol exhibit comparable efficacy in preventing postoperative delirium in elderly patients. However, remimazolam demonstrates superior hemodynamic stability and a reduced incidence of sleep disturbances, potentially enhancing overall patient outcomes. These findings support the preferential use of remimazolam in high-risk populations, though further large-scale randomized controlled trials are warranted to confirm these benefits and refine clinical recommendations.
Trial registration: The study protocol has been registered in PROSPERO (CRD42024600708).
Supplementary Information: The online version contains supplementary material available at 10.1186/s12871-025-03167-y.
Keywords: Delirium; Elderly patients; Meta-analysis; Propofol; Remimazolam.
Conflict of interest statement
Declarations. Content: All authors give consent for the publication of the manuscript. Presentation: None. Competing interests: The authors declare no competing interests.
Figures
References
-
- Maldonado JR. Acute brain failure: pathophysiology, diagnosis, management, and sequelae of Delirium. Crit Care Clin. 2017;33(3):461–519. - PubMed
-
- Kotfis K, Marra A, Ely EW. ICU delirium - a diagnostic and therapeutic challenge in the intensive care unit. Anaesthesiol Intensive Ther. 2018;50(2):160–7. - PubMed
-
- Rudy M, Saller T. [Postoperative delirium in the recovery room]. Die Anaesthesiologie. 2023;72(7):459–66. - PubMed
-
- D’Andria Ursoleo J, Bottussi A, Monaco F. Talk before they sleep: strategies for patient-centred communication in anaesthesiology. Br J Anaesth. 2024;133(5):934–9. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
