

Propofol-assisted deep extubation in the dental treatment of pediatrics: a randomized controlled triple-blind trial
- PMID: 40597652
- PMCID: PMC12210731
- DOI: 10.1186/s12871-025-03170-3
Propofol-assisted deep extubation in the dental treatment of pediatrics: a randomized controlled triple-blind trial
Abstract
Objectives: To verify whether propofol-assisted deep extubation is associated with fewer complications in pediatric patients undergoing dental treatment.
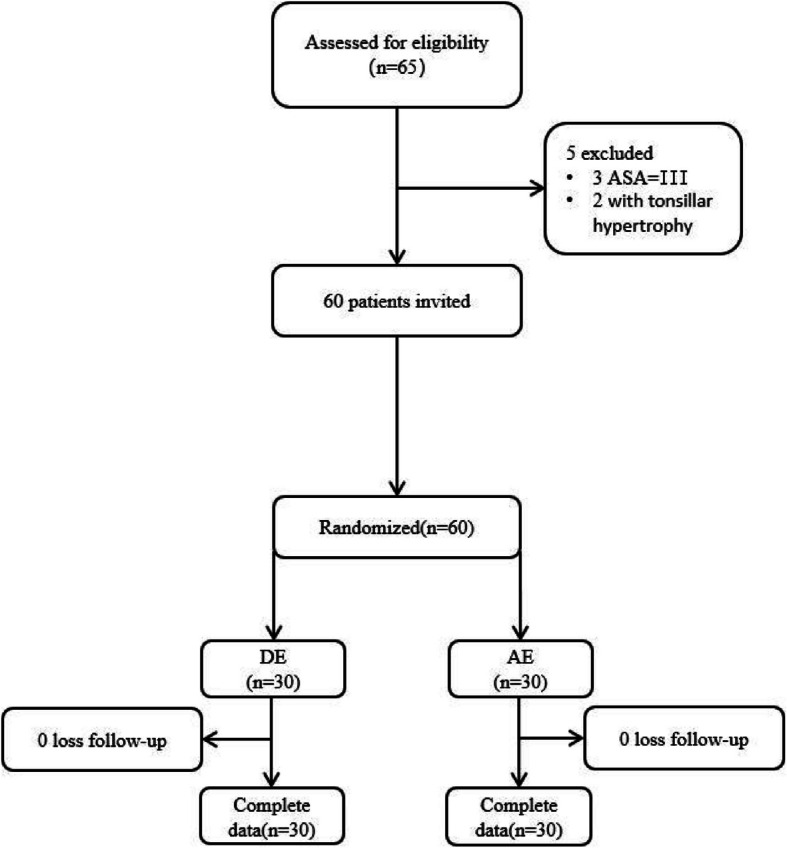
Materials and methods: This prospective study enrolled 60 pediatric candidates undergoing elective dental interventions, with randomized allocation to either deep extubation (DE; n = 30) or awake extubation (AE; n = 30) protocols. The primary endpoint was the incidence of at least 1 respiratory adverse event, whereas time to extubation (TOE), time to wake-up (TOW), hemodynamic fluctuations during extubation, incidence of emergence agitation (EA), nasal obstruction, epistaxis, sore throat, and hoarse voice after extubation were the secondary endpoints.
Results: The DE group reported significantly lower incidence of at least 1 respiratory adverse event (0.0% VS 23.3%, P = 0.016). The TOE was significantly shorter in the DE group, averaging 2.78 ± 0.87 min, compared to 5.50 ± 1.01 min in the AE group (P < .001). The TOW was longer in the DE group, with an average of 15.03 ± 3.44 min compared to 10.63 ± 1.52 min in the AE group (P < .001). The average value of mean arterial pressure (AVMAP) during extubation was lower in the DE group at 74.70 ± 13.35 mmHg, compared to 87.43 ± 15.31 mmHg in the AE group (P < .001). The average value of heart rate (AVHR) in the DE group was 108.37 ± 13.41 bpm, while in the AE group, it was 127.93 ± 20.74 bpm (P < .001). Additionally, the rates of sore throat and hoarse voice were significantly lower in the DE group (6.7% and 3.3%) than in the AE group (27% and 30%).
Conclusions: For pediatric patients undergoing dental treatment, propofol-assisted deep extubation is superior, allowing for less extubation time without increasing airway complications. This technique provides a smoother extubation with fewer hemodynamic fluctuations and lower incidences of voice hoarseness and persistent coughing, provided that certain rules for deep extubation are followed.
Keywords: Deep extubation; General anesthesia; Mouth rehabilitation.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Ethical approval for the present RCT was provided by the Ethics Committee of Baoding Second Hospital (no. KY2023044). The study was registered at www.chictr.org.cn (no. ChiCTR2400079951), and informed written consent was obtained from the legal guardians of all included participants before the study. All methods were performed in accordance with the relevant guidelines and regulations of the Helsinki Declaration. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Similar articles
-
A comparison of deep versus awake tracheal extubation in adults: a randomized controlled trial.BMC Anesthesiol. 2025 Jul 31;25(1):387. doi: 10.1186/s12871-025-03224-6. BMC Anesthesiol. 2025. PMID: 40745279 Free PMC article. Clinical Trial.
-
Effect of propofol combined with remimazolam besylate on blood pressure during general anesthesia induction in patients undergoing gynecological laparoscopic surgery: single-centre randomized controlled trial.BMC Anesthesiol. 2025 May 29;25(1):273. doi: 10.1186/s12871-025-03156-1. BMC Anesthesiol. 2025. PMID: 40442585 Free PMC article. Clinical Trial.
-
Remimazolam is more suitable for general anesthesia bronchoscopy in tuberculosis patients treated with isoniazid: a retrospective cohort analysis.BMC Anesthesiol. 2025 Aug 9;25(1):403. doi: 10.1186/s12871-025-03292-8. BMC Anesthesiol. 2025. PMID: 40783679 Free PMC article.
-
Early surfactant administration with brief ventilation vs. selective surfactant and continued mechanical ventilation for preterm infants with or at risk for respiratory distress syndrome.Cochrane Database Syst Rev. 2007 Oct 17;2007(4):CD003063. doi: 10.1002/14651858.CD003063.pub3. Cochrane Database Syst Rev. 2007. PMID: 17943779 Free PMC article.
-
Videolaryngoscopy versus direct laryngoscopy for adult patients requiring tracheal intubation.Cochrane Database Syst Rev. 2016 Nov 15;11(11):CD011136. doi: 10.1002/14651858.CD011136.pub2. Cochrane Database Syst Rev. 2016. Update in: Cochrane Database Syst Rev. 2022 Apr 4;4:CD011136. doi: 10.1002/14651858.CD011136.pub3. PMID: 27844477 Free PMC article. Updated.
References
-
- Sasaki CT, Suzuki M. Laryngeal spasm: a neurophysiologic redefinition. Ann Otol Rhinol Laryngol. 1977;86(2 pt. 1):150–7. - PubMed
-
- Ramgolam A, Hall GL, Zhang G, Hegarty M, von Ungern-Sternberg BS. Deep or awake removal of laryngeal mask airway in children at risk of respiratory adverse events undergoing tonsillectomy-a randomised controlled trial. Br J Anaesth. 2018;120(3):571–80. - PubMed
-
- von Ungern-Sternberg BS, Davies K, Hegarty M, Erb TO, Habre W. The effect of deep vs. awake extubation on respiratory complications in high-risk children undergoing adenotonsillectomy: a randomised controlled trial. Eur J Anaesthesiol. 2013;30(9):529–36. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
