

Incidence and predictors of discrepancies in radiology resident interpretations of coronary CT in the emergency department
- PMID: 40597776
- PMCID: PMC12220058
- DOI: 10.1186/s12880-025-01781-3
Incidence and predictors of discrepancies in radiology resident interpretations of coronary CT in the emergency department
Abstract
Background: Discrepancies between preliminary reports by on-call radiology residents and final reports of coronary computed tomography angiography (CCTA) in the emergency department (ED) have not been thoroughly investigated.
Methods: We conducted a retrospective quality assurance analysis of CCTA examinations performed during off-hours in a level-1 ED at a tertiary teaching hospital between March 2020 and April 2022. Discrepancies in identifying significant coronary artery disease (≥ 50% stenosis) between preliminary reports by on-call residents and final reports by board-certified cardiac radiologists were evaluated.
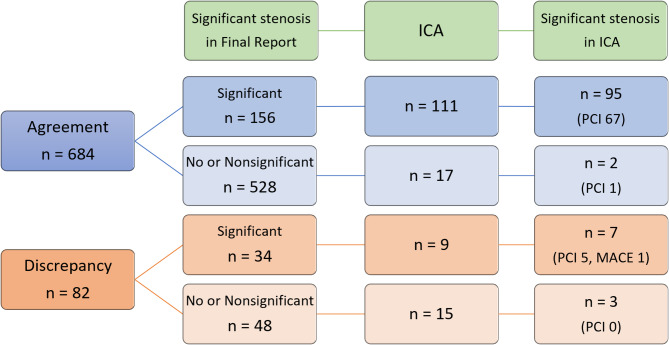
Results: Among the 766 patient visits (median age, 59 years [interquartile range, 47-70]; 415 men), 82 cases (10.7%) showed discrepancies. Univariable logistic regression analyses identified HEART score, day of ED visit, ED crowding index, and coronary artery calcium (CAC) score as significant factors associated with discrepancies. Multivariable analysis revealed that an ED crowding index < 40 (adjusted odds ratio = 2.06; P = 0.005), and positive CAC scores were independently associated with increased discrepancies (adjusted odds ratio = 4.56 for scores > 0 and ≤ 100, P < 0.001; 4.79 for scores > 100 and ≤ 400, P < 0.001; 3.69 for scores > 400, P = 0.002). The rate of unnecessary invasive coronary angiography was significantly higher in the discrepancy group (80.0%, 12 of 15) compared to the agreement group (14.4%, 16 of 111) (P < 0.05).
Conclusions: A substantial discrepancy rate was observed between preliminary and final CCTA interpretations in the ED. A lower ED crowding index and positive CAC scores were independently associated with an increased risk of discrepancies.
Keywords: Acute chest pain; Coronary computed tomography angiography; Discrepancy; Emergency department; Radiology resident.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was conducted in accordance with the Declaration of Helsinki. The institutional review board of Severance Hospital approved this study and waived the requirement for informed consent (IRB 4-2023-0702). Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures


References
-
- Gulati M, Levy PD, Mukherjee D, Amsterdam E, Bhatt DL, Birtcher KK, Blankstein R, Boyd J, Bullock-Palmer RP, Conejo T et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;144(22):e368-e454. - PubMed
-
- Kontos MC, de Lemos JA, Deitelzweig SB, Diercks DB, Gore MO, Hess EP, McCarthy CP, McCord JK, Musey PI Jr., Villines TC, et al. 2022 ACC expert consensus decision pathway on the evaluation and disposition of acute chest pain in the emergency department: A report of the American college of cardiology solution set oversight committee. J Am Coll Cardiol. 2022;80(20):1925–60. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
