

Development and validation of a risk nomogram predicting pneumothorax requiring chest tube placement post-percutaneous CT-guided lung biopsy
- PMID: 40597819
- PMCID: PMC12211772
- DOI: 10.1186/s12880-025-01794-y
Development and validation of a risk nomogram predicting pneumothorax requiring chest tube placement post-percutaneous CT-guided lung biopsy
Abstract
Background: Pneumothorax requiring chest tube after CT-guided transthoracic lung biopsy presents added clinical risk and costs to the healthcare system. Identifying high-risk patients can prompt alternative biopsy modes and/or better preparation for more focused post-procedural care. We aimed to develop and externally validate a risk nomogram for pneumothorax requiring chest tube placement following CT-guided lung biopsy, leveraging quantitative emphysema algorithm.
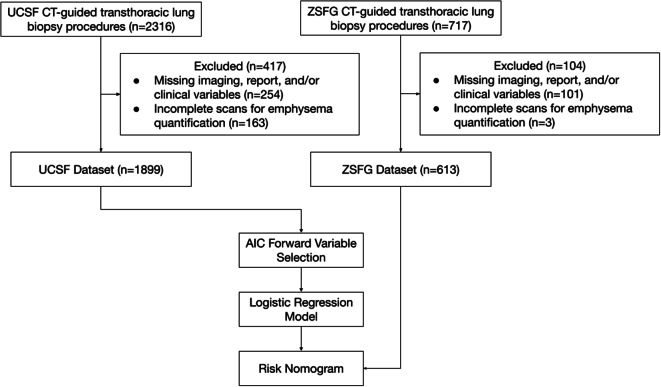
Methods: This two-center retrospective study included patients who underwent CT-guided lung biopsy from between 1994 and 2023. Data from one hospital was set aside for validation (n = 613). Emphysema severity was quantified and categorized to 3-point scale using a previously published algorithm based on 3×3×3 kernels and Hounsfield thresholding, and a risk calculator was developed using forward variable selection and logistic regression. The model was validated using bootstrapping and Harrell's C-index.
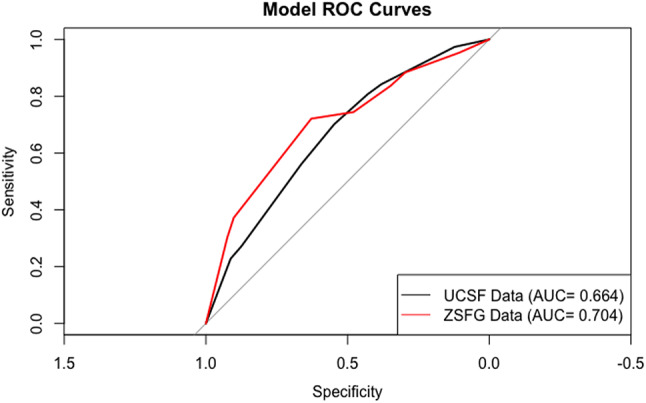
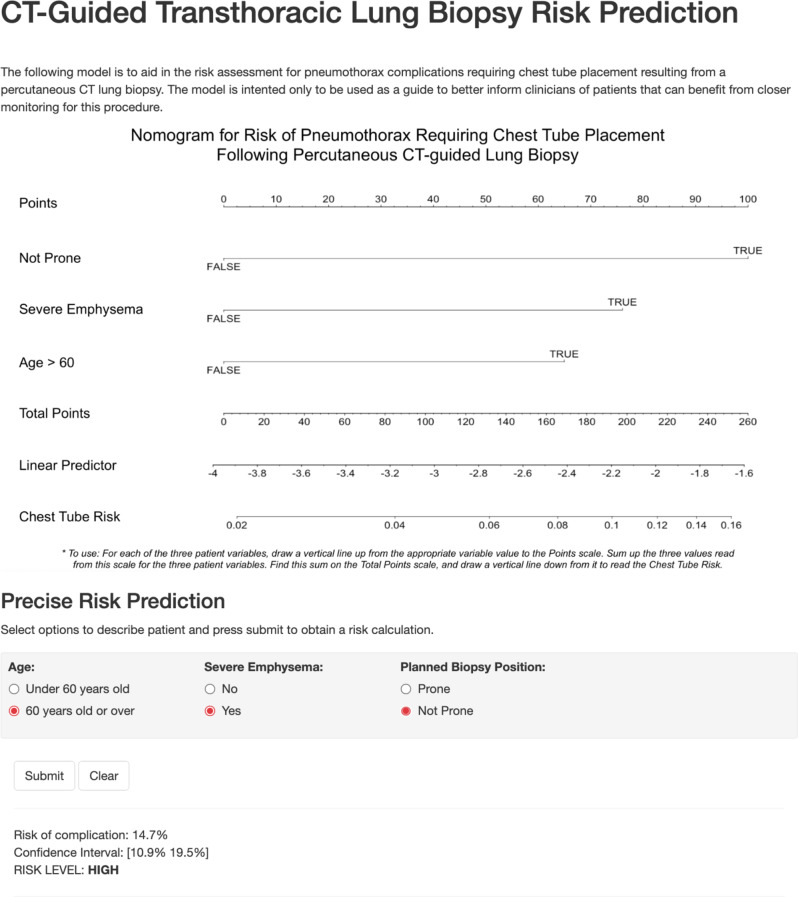
Results: 2,512 patients (mean age, 64.47 years ± 13.38 [standard deviation]; 1250 men) were evaluated, of whom 157 (6.7%) experienced pneumothorax complications requiring chest tube placement. After forward variable selection to reduce the covariates to maximize clinical usability, the risk score was developed using age over 60 (OR 1.80 [1.15-2.93]), non-prone patient position (OR 2.48 [1.63-3.75]), and severe emphysema (OR 1.99 [1.35-2.94]). The nomogram showed a mean absolute error of 0.5% in calibration and Harrell's C-index of 0.664 in discrimination in the internal cohort.
Conclusion: The developed nomogram predicts age over 60, non-prone position during biopsy, and severe emphysema to be most predictive of pneumothorax requiring chest tube placement following CT-guided lung biopsy.
Keywords: Image-guided biopsy; Lung neoplasms; Pneumothorax.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This retrospective study was conducted in accordance with the ethical standards of the institutional and national research committees and with the Helsinki Declaration and its later amendments or comparable ethical standards. The University of California, San Francisco Institutional Review Board approved the study (reference #: 422008), and the requirement for informed consent was waived. A clinical trial registration number is not applicable. Consent for publication: Not applicable. Competing interests: No competing interests.
Figures
Similar articles
-
Efficacy of autologous blood patch injection for pneumothorax rate after CT-guided percutaneous transthoracic lung biopsy: a systematic review and meta-analysis.J Cardiothorac Surg. 2024 Jun 14;19(1):332. doi: 10.1186/s13019-024-02781-0. J Cardiothorac Surg. 2024. PMID: 38877547 Free PMC article.
-
Effect of Saline Sealing After CT-Guided Lung Biopsy on Pneumothorax and Hemoptysis.J Comput Assist Tomogr. 2025 Jul-Aug 01;49(4):640-645. doi: 10.1097/RCT.0000000000001725. Epub 2025 Jan 27. J Comput Assist Tomogr. 2025. PMID: 39876517
-
Autologous blood patch intraparenchymal injection reduces the incidence of pneumothorax and the need for chest tube placement following CT-guided lung biopsy: a systematic review and meta-analysis.Eur J Med Res. 2024 Feb 9;29(1):108. doi: 10.1186/s40001-024-01707-9. Eur J Med Res. 2024. PMID: 38336678 Free PMC article.
-
The role of gravitational effects and pre-puncture techniques in reducing pneumothorax during CT-guided lung biopsies.Radiol Med. 2025 Jul;130(7):1024-1038. doi: 10.1007/s11547-025-02007-w. Epub 2025 Apr 15. Radiol Med. 2025. PMID: 40232655 Free PMC article.
-
Ultrasound versus computed tomography-guided transthoracic biopsy for pleural and peripheral lung lesions: a systematic review and meta-analysis.Acta Radiol. 2023 Dec;64(12):2999-3008. doi: 10.1177/02841851231206349. Epub 2023 Oct 12. Acta Radiol. 2023. PMID: 37822264
References
-
- Tomiyama N, Yasuhara Y, Nakajima Y, et al. CT-guided needle biopsy of lung lesions: A survey of severe complication based on 9783 biopsies in Japan. Eur J Radiol. 2006;59:60–64. 10.1016/j.ejrad.2006.02.001. - PubMed
-
- Weon J, Robson S, Chan R, Ussher S. Development of a risk prediction model of pneumothorax in percutaneous computed tomography guided transthoracic needle lung biopsy. J Med Imaging Radiat Oncol. 2021;65:686–93. 10.1111/1754-9485.13187. - PubMed
-
- Drumm O, Joyce EA, de Blacam C, et al. CT-guided lung biopsy: Effect of biopsy-side down position on pneumothorax and chest tube placement. Radiology. 2019;292:190–96. 10.1148/radiol.2019182321. - PubMed
