

Early assessment of therapeutic efficacy in lymphoma patients via a blood-based multi-omics response monitoring test
- PMID: 40597857
- PMCID: PMC12210469
- DOI: 10.1186/s12885-025-14457-6
Early assessment of therapeutic efficacy in lymphoma patients via a blood-based multi-omics response monitoring test
Abstract
Background: Periodic fluorodeoxyglucose (FDG) positron emission tomography (PET)-computed tomography (CT)/CT-based response examinations are the current standard for clinical assessment of lymphoma treatment response. In this prospective study, we applied a blood-based multi-omics test, SeekInClarity, to assess treatment response and to predict therapeutic outcomes in the major lymphoma subtypes.
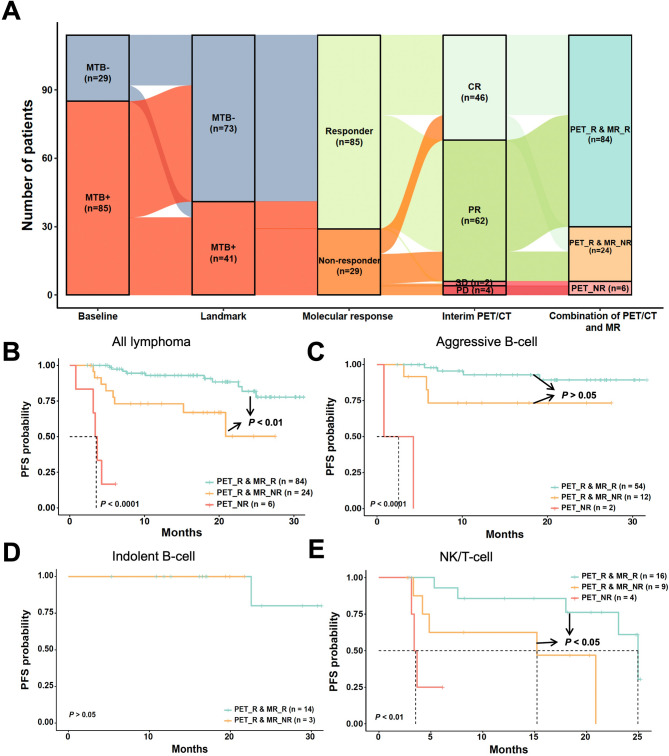
Methods: We prospectively recruited 116 lymphoma patients from two clinical centers, and collected blood samples at pre-treatment (baseline) and after two treatment cycles (landmark) to calculate molecular tumor burden (MTB) score using SeekInClarity. The "molecular response" framework, developed based on the MTB dynamic changes between baseline and landmark, was used to predict prompt treatment efficacy across various first-line regimens.
Results: Higher MTB scores correlated with advanced tumor stages, with MTB+ ratios of 31.8%, 63.6%, 84.6%, and 91.2% for stage I, II, III, and IV respectively. At landmark, MTB+ patients (n = 41) exhibited significantly worse progression-free survival (PFS, HR 7.78, 95% CI 3.00-20.18, P < 0.0001) and overall survival (OS, HR 4.14, 95% CI 1.03-16.59, P < 0.05) compared to the MTB- patients (n = 75). Multivariable Cox regression analysis demonstrated that only molecular response and interim PET/CT were independent predictor of treatment outcome, outperforming the clinical biomarkers B2M and LDH. Among the 108 patients with interim PET/CT response, SeekInClarity further identified 24 (22.2%) patients as molecular non-responders. Of these, 8 (33.3%) patients experienced disease progression within 27.5 months, while only 10 (11.9%) patients among the remaining 84 molecular responders progressed within 31.7 months. This significant difference indicated that molecular non-responders have notably worse PFS than molecular responders (P < 0.01), particularly in aggressive B-cell and NK/T-cell lymphomas. These findings underscore the added value of molecular profiling in refining risk stratification beyond imaging alone.
Conclusions: The SeekInClarity-based molecular response predicts prompt treatment efficacy and serves as a valuable complementary tool for identifying non-responders among interim PET/CT response patients.
Keywords: Efficacy assessment; Liquid biopsy; Lymphoma; Molecular response; Multi-omics.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by the Ethics Committee of The First Affiliated Hospital of Zhengzhou University (2022-KY-0719-001). All experiments and procedures were conducted in accordance with relevant guidelines, regulations, local standards, and institutional requirements. Written informed consent was obtained from all participants before they participated in the study. Consent for publication: Not applicable. Competing interests: S. Li, W. Wu, and M. Mao are full-time employees and stock shareholders of SeekIn Inc. Y. Chang and D. Zhu are full-time employees of Shenyou Bio, a wholly-owned subsidiary of SeekIn Inc, and hold stock options in SeekIn Inc. F. Chang and D. Gong are full-time employee of Shenyou Bio. Other authors declare no potential conflicts of interest.
Figures



References
-
- Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17–48. 10.3322/caac.21763. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
