

The probability of lung cancer in patients with pulmonary nodules detected via low-dose computed tomography screening in China
- PMID: 40597901
- PMCID: PMC12210631
- DOI: 10.1186/s12885-025-14449-6
The probability of lung cancer in patients with pulmonary nodules detected via low-dose computed tomography screening in China
Abstract
Objective: Low dose computed tomography (LDCT) screening has been proven to be effective in reducing lung cancer mortality, but the ensuing high false-positive and overdiagnosis rates shackle the effectiveness of lung cancer screening (LCS) in China. Nodule malignancy prediction models may be an applicable solution.
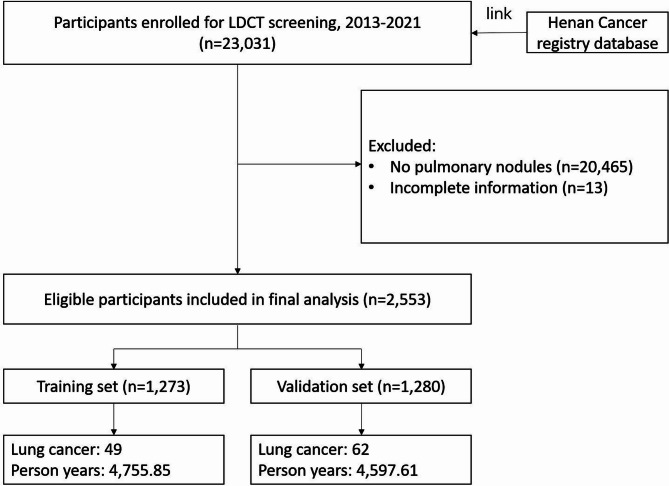
Methods: We conducted a prospective cohort study to develop and internally validate the model using data from the ongoing Henan province Cancer Screening Program in Urban China (CanSPUC). From 2013 to 2021, 23,031 heavy smokers underwent baseline screening with LDCT; 2553 participants were diagnosed with pulmonary nodules. Detailed questionnaire, physical assessment and follow-up were completed for all participants. Multivariable Cox proportional risk regression models were used to identify and integrate key prognostic factors for the development of a nomogram model. Data from the National Lung Screening Trial (NLST) were utilized for external validation.
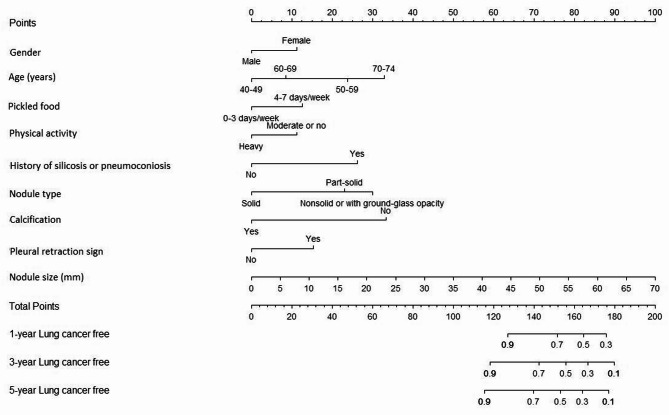
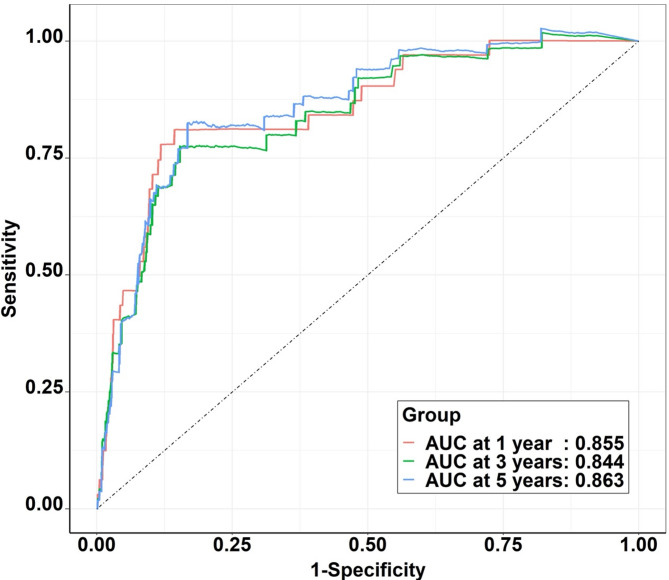
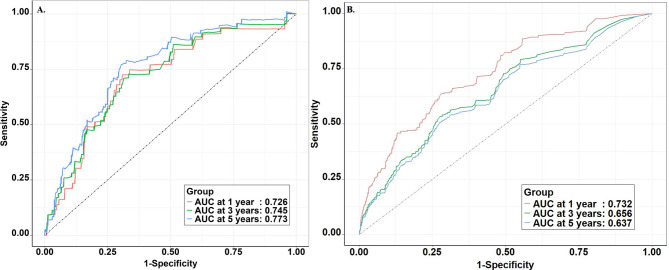
Results: A total of 111 lung cancer cases with a median follow-up duration of 3.7 years occurred in the Henan CanSPUC. Age, gender, physical activity, consumption of pickled food, history of silicosis or pneumoconiosis, nodule type, size, calcification, and pleural retraction sign were included into the model. The AUC was 0.855, 0.844, and 0.863 for the 1-, 3- and 5-year lung cancer risk in the training set, respectively. Compared with Mayo model, VA model, PKU model, and Brock model, the Henan CanSPUC model yield statistically better discriminatory performance (all P values < 0.05). The model calibrated well across the deciles of predicted risk in both the overall population and all subgroups. The model demonstrated good calibration and discrimination in the internal validation cohort, while the external validation cohort showed lower predictive performance, indicating that further external validation is needed.
Conclusions: The model developed and validated in this study may be used to estimate the probability of lung cancer in nodules detected at baseline LDCT, allowing more efficient risk-adapted follow-up in population-based LCS programs. However, further external validation in broader and more diverse populations is warranted.
Keywords: Lung Cancer; Prospective screening cohort; Pulmonary nodules; Risk assessment.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was conducted following the guidelines of the Helsinki Declaration and was approved by the Medical Ethics Committee of the Henan Cancer Hospital. Written informed consent forms were obtained from all participants. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests. Role of the funder: The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Figures
Similar articles
-
Impact of low-dose computed tomography (LDCT) screening on lung cancer-related mortality.Cochrane Database Syst Rev. 2022 Aug 3;8(8):CD013829. doi: 10.1002/14651858.CD013829.pub2. Cochrane Database Syst Rev. 2022. PMID: 35921047 Free PMC article.
-
External validation of the performance of commercially available deep-learning-based lung nodule detection on low-dose CT images for lung cancer screening in Japan.Jpn J Radiol. 2025 Apr;43(4):634-640. doi: 10.1007/s11604-024-01704-2. Epub 2024 Nov 30. Jpn J Radiol. 2025. PMID: 39613978 Free PMC article.
-
Development and interpretation of machine learning-based prognostic models for predicting high-risk prognostic pathological components in pulmonary nodules: integrating clinical features, serum tumor marker and imaging features.J Cancer Res Clin Oncol. 2025 Jun 17;151(6):190. doi: 10.1007/s00432-025-06241-7. J Cancer Res Clin Oncol. 2025. PMID: 40524012 Free PMC article.
-
The effectiveness and cost-effectiveness of carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma: a systematic review and economic evaluation.Health Technol Assess. 2007 Nov;11(45):iii-iv, ix-221. doi: 10.3310/hta11450. Health Technol Assess. 2007. PMID: 17999840
-
A Predictive Model Integrating AI Recognition Technology and Biomarkers for Lung Nodule Assessment.Thorac Cardiovasc Surg. 2025 Mar;73(2):174-181. doi: 10.1055/a-2446-9832. Epub 2024 Nov 26. Thorac Cardiovasc Surg. 2025. PMID: 39591993 Free PMC article.
References
-
- Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–63. - PubMed
-
- Passiglia F, Cinquini M, Bertolaccini L, Del Re M, Facchinetti F, Ferrara R, et al. Benefits and harms of lung Cancer screening by chest computed tomography: A systematic review and Meta-Analysis. J Clin Oncol. 2021;39(23):2574–85. - PubMed
-
- De Koning HJ, Van Der Aalst CM, De Jong PA, Scholten ET, Nackaerts K, Heuvelmans MA, et al. Reduced Lung-Cancer mortality with volume CT screening in a randomized trial. N Engl J Med. 2020;382(6):503–13. - PubMed
MeSH terms
Grants and funding
- 2023M731010/China Postdoctoral Science Foundation
- YXKC2022045/the Training Project for Young and Middle-aged Excellent Talents in Health Science and Technology Innovation of Henan Province
- 221111310200/the Henan Province key research and development project
- No.82204121/Natural Science Foundation of China
LinkOut - more resources
Full Text Sources
Medical
