

Comparison of double-layered scallop-shaped anastomosis and circular stapled anastomosis in Ivor-Lewis surgery for esophageal and EGJ cancer: a retrospective cohort study
- PMID: 40597983
- PMCID: PMC12211163
- DOI: 10.1186/s12885-025-14437-w
Comparison of double-layered scallop-shaped anastomosis and circular stapled anastomosis in Ivor-Lewis surgery for esophageal and EGJ cancer: a retrospective cohort study
Abstract
Background: Cancers of the lower esophagus and esophagogastric junction (EGJ) are highly aggressive and have poor prognoses. Minimally invasive Ivor-Lewis surgery (MIIL) is the preferred treatment, but anastomotic leakage (AL) remains a critical complication of this procedure. In the present study, we introduce a novel double-layered scallop-shaped anastomosis (DLSSA) technique and compare its outcomes with those of circular stapled esophagogastric anastomosis (CSEA).
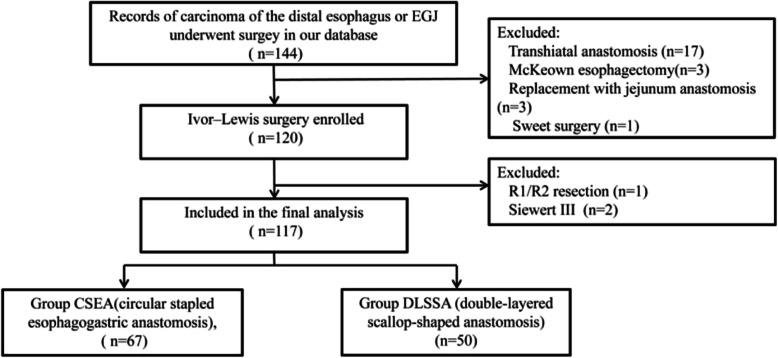
Methods: From April 2016 to February 2023, 117 patients with distal esophageal or EGJ cancer who underwent complete thoracoscopic-laparoscopic Ivor-Lewis surgery were retrospectively analyzed. Patients were divided into DLSSA (n = 50) and CSEA (n = 67) groups. The median value and ranges are used to present the numerical data. Continuous and categorical variables were compared between groups with the Kruskal‒Wallis test and Fisher's exact test or χ2 test, respectively. Multivariable binary logistic regression analyses were performed to identify potential prognostic factors.
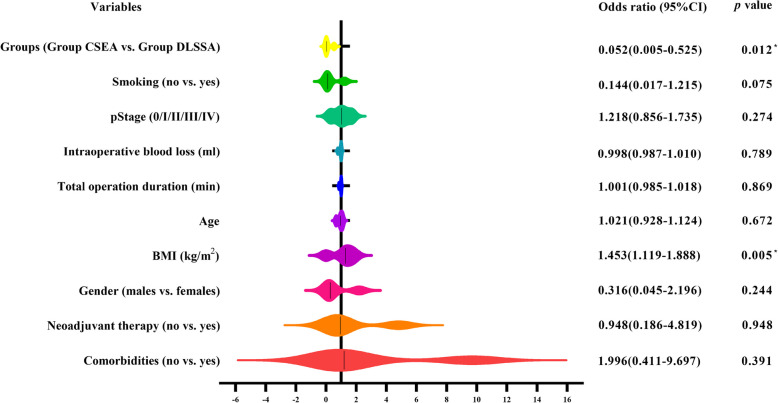
Results: The median total operation duration was similar between the groups (280 min). Intraoperative blood loss was slightly greater in the CSEA group (120 ml vs. 100 ml, p = 0.001). Postoperative complications occurred in 32.5% of the patients, with no significant between-group difference. However, the incidence of AL was significantly lower (4.0% vs. 17.9%, p = 0.022) and that of pleural effusion was significantly greater (10.0% vs. 1.5%, p = 0.039) in the DLSSA group than in the CSEA group. Multivariable analysis revealed that a higher body mass index (OR = 1.453, 95% CI: 1.119-1.888; p = 0.005) was a risk factor for AL, whereas undergoing DLSSA was associated with reduced AL risk (OR = 0.052, 95% CI: 0.005-0.525; p = 0.012), and both variables were considered independent predictors of AL risk.
Conclusion: Compared with CSEA, DLSSA was associated with significantly lower risk of AL in thoracoscopic Ivor-Lewis surgery, demonstrating its potential as a safer anastomotic technique. However, its association with increased pleural effusion warrants further investigation. Prospective randomized trials are needed to validate long-term outcomes and optimize procedural efficacy.
Keywords: Carcinoma; Esophagogastric junction; Ivor–Lewis; Postoperative complications; Scallop-shaped anastomosis.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was conducted in accordance with the ethical principles of the Declaration of Helsinki and its later amendments. Prior to the operations, patients were informed about the procedures and provided their consent. Ethical approval for the study was obtained from the Ethics Committee of Daping Hospital and Research Institute of Surgery, Army Military Medical University (Ethics ID: 2020–157). Written informed consent was obtained from all individual participants prior to their inclusion in the study. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. - PubMed
-
- Li KK, Bao T, Wang YJ, Liu XH, Guo W. The Postoperative outcomes of thoracoscopic-laparoscopic Ivor-Lewis surgery plus D2 celiac lymphadenectomy for patients with adenocarcinoma of the esophagogastric junction. Surg Endosc. 2019; 34(11):4957–66. - PubMed
-
- Haverkamp L, Seesing MF, Ruurda JP, Boone J, Hillegersberg RV. Worldwide trends in surgical techniques in the treatment of esophageal and gastroesophageal junction cancer. Dis Esophagus. 2017;30(1):1–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
