

CAR-T cells targeting CCR9 and CD1a for the treatment of T cell acute lymphoblastic leukemia
- PMID: 40598348
- PMCID: PMC12220514
- DOI: 10.1186/s13045-025-01715-0
CAR-T cells targeting CCR9 and CD1a for the treatment of T cell acute lymphoblastic leukemia
Abstract
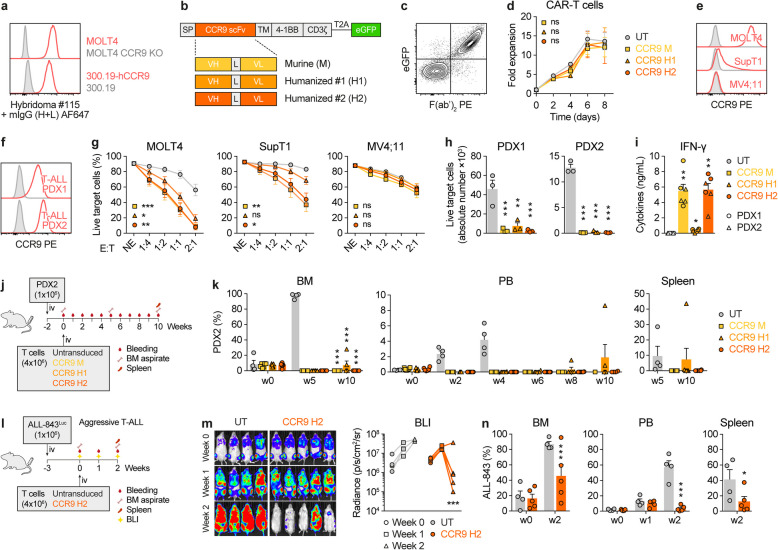
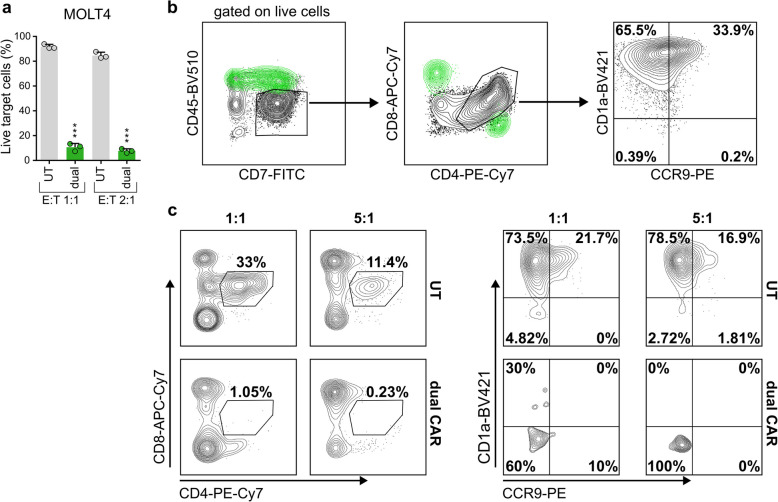
T cell acute lymphoblastic leukemia (T-ALL) is an aggressive malignancy characterized by high rates of induction failure and relapse, and effective targeted immunotherapies are lacking. Despite promising clinical progress with genome-edited CD7-directed CAR-T cells, which present significant logistical and regulatory issues, CAR-T cell therapy in T-ALL remains challenging due to the shared antigen expression between malignant and healthy T cells. This can result in CAR-T cell fratricide, T cell aplasia, and the potential for blast contamination during CAR-T cell manufacturing. Recently described CAR-T cells target non-pan-T antigens, absent on healthy T cells but expressed on specific T-ALL subsets. These antigens include CD1a (NCT05679895), which is expressed in cortical T-ALL, and CCR9. We show that CCR9 is expressed on >70% of T-ALL patients (132/180) and is maintained at relapse, with a safe expression profile in healthy hematopoietic and non-hematopoietic tissues. Further analyses showed that dual targeting of CCR9 and CD1a could benefit T-ALL patients with a greater blast coverage than single CAR-T cell treatments. We therefore developed, characterized, and preclinically validated a novel humanized CCR9-specific CAR with robust and specific antileukemic activity as a monotherapy in vitro and in vivo against cell lines, primary T-ALL samples, and patient-derived xenografts. Importantly, CCR9/CD1a dual-targeting CAR-T cells showed higher efficacy than single-targeting CAR-T cells, particularly in T-ALL cases with phenotypically heterogeneous leukemic populations. Dual CD1a/CCR9 CAR-T therapy may prevent T cell aplasia and obviate the need for allogeneic transplantation and regulatory-challenging genome engineering approaches in T-ALL.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: PM is a cofounder of OneChain Immunotherapeutics, a spin-off company from the Josep Carreras Leukemia Research Institute which has licensed the CCR9 binder (PCT/EP2024/053734). The remaining authors report no conflicts of interest in this work.
Figures




References
-
- Litzow MR, Ferrando AA. How I treat T-cell acute lymphoblastic leukemia in adults. Blood. 2015;126:833–41. - PubMed
-
- Vora A, et al. Treatment reduction for children and young adults with low-risk acute lymphoblastic leukaemia defined by minimal residual disease (UKALL 2003): a randomised controlled trial. Lancet Oncol. 2013;14:199–209. - PubMed
-
- Schrappe M, et al. Late MRD response determines relapse risk overall and in subsets of childhood T-cell ALL: results of the AIEOP-BFM-ALL 2000 study. Blood. 2011;118:2077–84. - PubMed
-
- Fielding AK, et al. Outcome of 609 adults after relapse of acute lymphoblastic leukemia (ALL); an MRC UKALL12/ECOG 2993 study. Blood. 2007;109:944–50. - PubMed
MeSH terms
Substances
Grants and funding
- FPU19/00039/FPU Fellowship-Spanish Ministry of Science and Innovation
- 101153028/European Union's Marie Skłodowska-Curie Actions (MSCA) Postdoctoral Fellowship
- DIN2022-012556/Industrial PhD fellowship
- FJC2021-046789-I/Juan de la Cierva postdoctoral fellowship
- PRYGN211192BUEN/Fundación Científica Asociación Española Contra el Cáncer
- PRYGN211192BUEN/Fundación Científica Asociación Española Contra el Cáncer
- PRYGN211192BUEN/Fundación Científica Asociación Española Contra el Cáncer
- RD24/0014/0024/Instituto de Salud Carlos III (ISCIII) through the Spanish Network of Advanced Therapies (RICORS/TERAV+)
- RD24/0014/0015/Instituto de Salud Carlos III (ISCIII) through the Spanish Network of Advanced Therapies (RICORS/TERAV+)
- RD24/0014/0042/Instituto de Salud Carlos III (ISCIII) through the Spanish Network of Advanced Therapies (RICORS/TERAV+)
- PTQ2020-011056/Torres Quevedo contract
- PID2022-138880OB-I00/AEI
- PID2022-136554OA-I00/MICIU/AEI 10.13039/501100011033 and the European Regional Development Fund (ERDF)/EU
- ERC-PoC-957466 IT4B-TALL/ERC_/European Research Council/International
- 101057250-CANCERNA/H2020
- PID2022-142966OB-I00/MCIN/AEI/10.13039/501100011033 and FEDER Funds
- CPP2021-008508/MICIU/AEI/10.13039/501100011033 and the European Union NextGenerationEU/PRTR
LinkOut - more resources
Full Text Sources
Research Materials
