

Multisensory BCI promotes motor recovery via high-order network-mediated interhemispheric integration in chronic stroke
- PMID: 40598460
- PMCID: PMC12220625
- DOI: 10.1186/s12916-025-04214-8
Multisensory BCI promotes motor recovery via high-order network-mediated interhemispheric integration in chronic stroke
Abstract
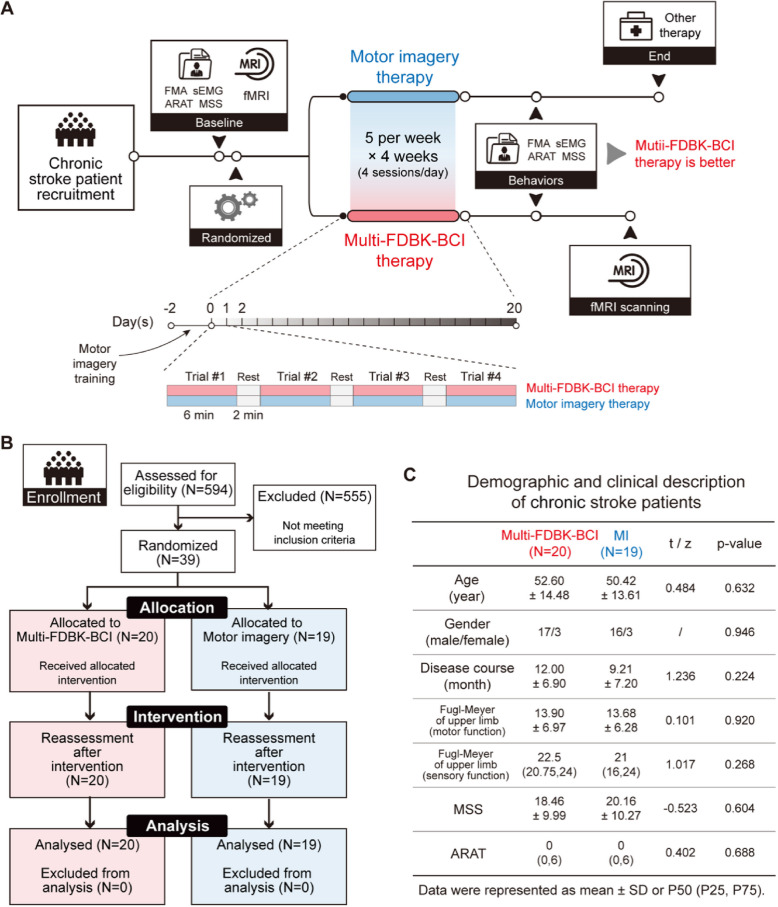
Background: Chronic stroke patients often experience persistent motor impairments, and current rehabilitation therapies rarely achieve substantial functional recovery. Sensory feedback during movement plays a pivotal role in driving neuroplasticity. This study introduces a novel multi-modal sensory feedback brain-computer interface (Multi-FDBK-BCI) system that integrates proprioceptive, tactile, and visual stimuli into motor imagery-based training. We aimed to explore the potential therapeutic efficacy and elucidate its neural mechanisms underlying motor recovery.
Methods: Thirty-nine chronic stroke patients were randomized to either the Multi-FDBK-BCI group (n = 20) or the conventional motor imagery therapy group (n = 19). Motor recovery was assessed using the Fugl-Meyer Assessment (primary outcome), Motor Status Scale, Action Research Arm Test, and surface electromyography. Functional MRI was used to examine brain activation patterns during upper limb tasks, while Granger causality analysis and machine learning evaluated inter-regional connectivity changes and their predictive value for recovery.
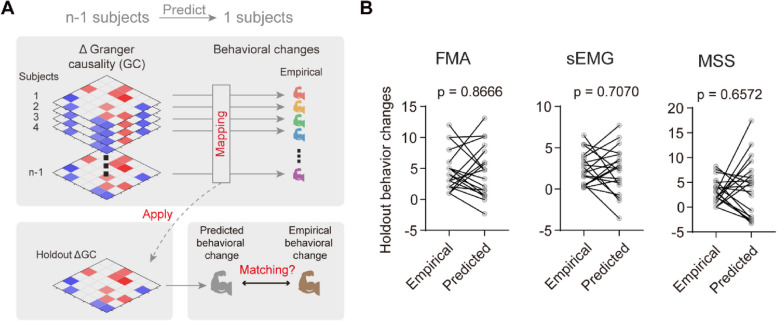
Results: Multi-FDBK-BCI training led to significantly greater motor recovery compared to conventional therapy. Functional MRI revealed enhanced activation of high-order transmodal networks-including the default mode, dorsal/ventral attention, and frontoparietal networks-during paralyzed limb movement, with activation strength positively correlated with motor improvement. Granger causality analysis identified a distinct information flow pattern: signals from the lesioned motor cortex were relayed through transmodal networks to the intact motor cortex, promoting interhemispheric communication. These functional connectivity changes not only supported motor recovery but also served as robust predictors of therapeutic outcomes.
Conclusions: Our findings highlight the Multi-FDBK-BCI system as a promising strategy for chronic stroke rehabilitation, leveraging activity-dependent neuroplasticity within high-order transmodal networks. This multi-modal approach holds significant potential for patients with limited recovery options and sheds new light on the neural drivers of motor restoration, warranting further investigation in clinical neurorehabilitation.
Trial registration: All data used in the present study were obtained from a research trial registered with the ClinicalTrials.gov database (ChiCTR-ONC-17010739, registered 26 February 2017, starting from 10 January 2017).
Keywords: Brain pasticity; Brain-computer interface; Hemiplegia; Multi-modal sensory feedback; Stroke.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by the Ethics Committee of Huashan Hospital (2017-016). All patients provided informed consent prior to participating in the trial. The study adhered to the principles of the declaration of Helsinki and was prospectively registered in a publicly accessible clinical trials registry ( https://www.chictr.org.cn/ , identifier: ChiCTR-ONC-17010739). Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures




Similar articles
-
Multimodal assessment of a BCI system for stroke rehabilitation integrating motor imagery and motor attempts: a randomized controlled trial.J Neuroeng Rehabil. 2025 Aug 26;22(1):185. doi: 10.1186/s12984-025-01723-8. J Neuroeng Rehabil. 2025. PMID: 40859358 Free PMC article. Clinical Trial.
-
Integrating Brain-Computer Interface Systems into Occupational Therapy for Enhanced Independence of Stroke Patients: An Observational Study.Medicina (Kaunas). 2025 May 21;61(5):932. doi: 10.3390/medicina61050932. Medicina (Kaunas). 2025. PMID: 40428890 Free PMC article.
-
Effects and neural mechanisms of a brain-computer interface-controlled soft robotic glove on upper limb function in patients with subacute stroke: a randomized controlled fNIRS study.J Neuroeng Rehabil. 2025 Jul 24;22(1):171. doi: 10.1186/s12984-025-01704-x. J Neuroeng Rehabil. 2025. PMID: 40707971 Free PMC article. Clinical Trial.
-
Use of Electroencephalography Brain-Computer Interface Systems as a Rehabilitative Approach for Upper Limb Function After a Stroke: A Systematic Review.PM R. 2017 Sep;9(9):918-932. doi: 10.1016/j.pmrj.2017.04.016. Epub 2017 May 13. PM R. 2017. PMID: 28512066
-
Yoga for stroke rehabilitation.Cochrane Database Syst Rev. 2017 Dec 8;12(12):CD011483. doi: 10.1002/14651858.CD011483.pub2. Cochrane Database Syst Rev. 2017. PMID: 29220541 Free PMC article.
References
-
- Duncan PW, Bushnell C, Sissine M, Coleman S, Lutz BJ, Johnson AM, Radman M, Pvru Bettger J, Zorowitz RD, Stein J. Comprehensive stroke care and outcomes: time for a paradigm shift. Stroke. 2021;52(1):385–93. - PubMed
-
- Kajrolkar T, Yang F, Pai YC, Bhatt T. Dynamic stability and compensatory stepping responses during anterior gait-slip perturbations in people with chronic hemiparetic stroke. J Biomech. 2014;47(11):2751–8. - PubMed
Publication types
MeSH terms
Grants and funding
- 82372570/the National Science Foundation of China
- 82372570/the National Science Foundation of China
- 82271422/the National Science Foundation of China
- 23Y11900900/Medical Innovation Research Project funded by Shanghai Science and Technology Commission
- 23Y11900900/Medical Innovation Research Project funded by Shanghai Science and Technology Commission
LinkOut - more resources
Full Text Sources
Medical
