

Cross-national differences in the association between estimated cardiorespiratory fitness and depressive symptoms among older adults: findings from three nationwide cohort studies
- PMID: 40598464
- PMCID: PMC12220467
- DOI: 10.1186/s12916-025-04175-y
Cross-national differences in the association between estimated cardiorespiratory fitness and depressive symptoms among older adults: findings from three nationwide cohort studies
Abstract
Background: Cardiorespiratory fitness (CRF) is a modifiable risk factor for chronic diseases, but its association with depressive symptoms remains unclear, particularly across different populations. We aimed to investigate the link between estimated CRF (eCRF) and incident depressive symptoms among individuals over 50 years old, and to explore potential cross-country variations in this association.
Methods: Data were retrieved from three national cohorts: the Health and Retirement Study (HRS, United States), the English Longitudinal Study of Ageing (ELSA, England), and the China Health and Retirement Longitudinal Study (CHARLS, China). eCRF was estimated using sex-specific algorithms and categorized into low (quintiles 1), moderate (quintiles 2-3), and high (quintiles 4-5) levels. Depressive symptoms were measured using the 8-item Center for Epidemiological Studies Depression Scale (CESD-8) (cutoff ≥ 3) in HRS and ELSA, and the 10-item version (CESD-10) (cutoff ≥ 10) in CHARLS. Cox proportional hazard models estimated hazard ratios (HRs) and 95% confidence intervals (CIs), adjusting for potential confounders.
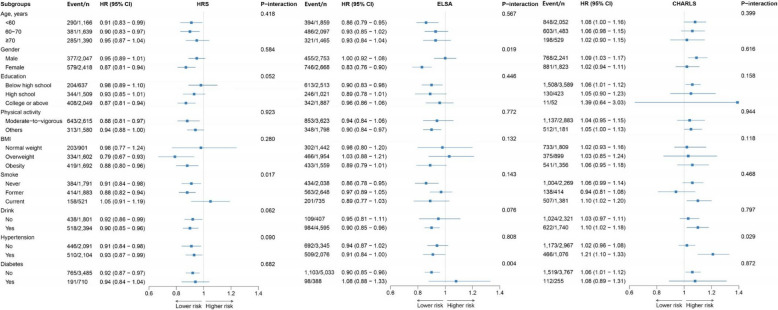
Results: This study included 13,680 participants (4195 from HRS, 5421 from ELSA, and 4064 from CHARLS) with median follow-ups of 9.78, 12.11, and 5.73 years, respectively. Depressive symptoms incidence was 22.79% in HRS, 22.15% in ELSA, and 40.58% in CHARLS. Per 1-SD increase in eCRF was associated with 9% lower risk of depressive symptoms in HRS (HR = 0.91; 95% CI, 0.87-0.96), 8% lower in ELSA (HR = 0.92; 95% CI, 0.87-0.97), but 6% higher in CHARLS (HR = 1.06; 95% CI, 1.01-1.16). Compared with the low eCRF level group, high eCRF level was associated with decreased risk of depressive symptoms in HRS (HR = 0.69; 95% CI, 0.55-0.85) and ELSA (HR = 0.62; 95% CI, 0.48-0.79), but increased risk in CHARLS (HR = 1.27; 95% CI, 1.01-1.61). Subgroup analyses revealed that the associations were modified by smoking status (HRS), by gender and presence of diabetes (ELSA), and by the presence of hypertension (CHARLS) (P for interaction < 0.05).
Conclusions: A higher level of eCRF was associated with reduced depressive symptoms risk in the US (HRS) and England (ELSA) older adults but with increased risk in China (CHARLS), emphasizing the need for nation-specific public health strategies.
Keywords: Cardiorespiratory fitness; Depressive symptoms; Nationwide cohort studies; Older adults.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The Health and Retirement Study is sponsored by the National Institute on Aging (grant number NIA U01 AG009740) and is conducted by the University of Michigan (IRB Protocol: HUM00061128 approved through 10/18/2018). Ethical approval for all the English Longitudinal Study of Ageing waves was granted from NHS Research Ethics Committees under the National Research and Ethics Service (NRES): wave 2 and wave 3 received ethical approval from the London Multi-Centre Research Ethics Committee on 12 th August 2004 (MREC/04/2/006) and 27 th October 2005 (05/MRE02/63); wave 4 received ethical approval from the National Hospital for Neurology and Neurosurgery & Institute of Neurology Joint Research Ethics Committee on 12 th October 2007 (07/H0716/48); wave 5 received ethical approval from the Berkshire Research Ethics Committee on 21 st December 2009 (09/H0505/124); wave 6 and wave 7 received ethical approval from the NRES Committee South Central—Berkshire on 28 th November 2012 (11/SC/0374) and 28 th November 2013 (13/SC/0532); wave 8 and wave 9 received ethical approval from the South Central – Berkshire Research Ethics Committee on 23rd September 2015 (15/SC/0526) and 10 th May 2018 (17/SC/0588). The China Health and Retirement Longitudinal Study was approved by the Biomedical Ethics Review Committee of Peking University (IRB00001052-14010). All participants provided written consent. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures


References
MeSH terms
Grants and funding
- KY0120220263/Guangdong Provincial People's Hospital Supporting Fund for Talent Program
- (82271125, 81870663 and 82171075/LiaoNing Revitalization Talents Program (XLYC2203192), National Natural Science Foundation of China
- 2023B1515120028/Basic and Applied Basic Research Foundation of Guangdong Province
- (8217040449, 8227040339 and 8217040546/the launch fund of Guangdong Provincial People's Hospital for NSFC
- 20220610092/the Science and Technology Program of Guangzhou
- KJ012019087/the Outstanding Young Talent Trainee Program of Guangdong Provincial People's Hospital
- KJ012019457/the GDPH Scientific Research Funds for Leading Medical Talents and Distinguished Young Scholars in Guangdong Province
- 2023-31/Personalized Medical Incubator Project, The fund for Precison Medicine Research and Industry Development in SIMQ
LinkOut - more resources
Full Text Sources
Medical
