

Comment
doi: 10.1186/s13054-025-05440-5.
Co-existence of congestion and preload-dependence identified by pulse pressure respiratory variations: right ventricular afterload might be the key
Affiliations
- PMID: 40598584
- PMCID: PMC12211315
- DOI: 10.1186/s13054-025-05440-5
Item in Clipboard
Comment
Co-existence of congestion and preload-dependence identified by pulse pressure respiratory variations: right ventricular afterload might be the key
Crit Care.
.
No abstract available
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
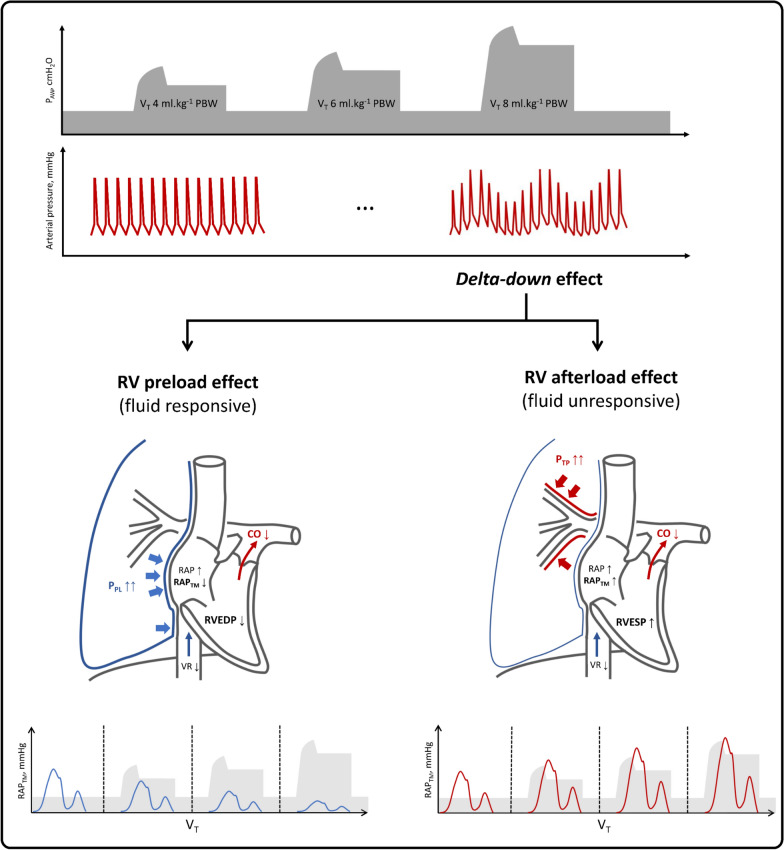
Transmural RAP patterns reveal distinct mechanisms behind PPV changes. Pulse pressure variation (PPV) may result from the presence of a delta-up component, a delta-down component, or both. The delta-down component, typically observed a few heartbeats after insufflation, reflects a decrease in cardiac output subsequent to cardio-respiratory interactions. This reduction may be driven by two distinct mechanisms, described in the figure using varying tidal volumes and their effects on right ventricular preload and afterload. First, an increase in pleural pressure during insufflation is transmitted to the pericardial space, resulting in an elevation of intra-luminal right atrial pressure but a reduction in transmural right atrial pressure (RAPtm). This rise in intra-luminal right atrial pressure impairs the venous return gradient, thereby contributing to the drop in RAPtm. Additionally, the increase in pleural pressure reduces the transmural pressure of the superior vena cava via a “waterfall” effect, further reducing RAPtm. As a result, end-systolic right atrial volume and venous return are reduced, accentuating the decrease in right ventricular preload during insufflation, being indicative of a preload responsive state. Oppositely, an increase in transpulmonary pressure during tidal volume insufflation may elevate pulmonary vascular resistance of non-zone 3 West zones and right ventricular afterload, thereby opposing right ventricular outflow. This backward pressure is transmitted to the right atrium, leading to an increase in both intra-luminal and transmural RAP and a decrease in venous return [4]. These conditions would correspond to a preload unresponsive state, despite significant PPV. Finally, these two patterns of cardio-respiratory interactions may probably coexist in a ventilated patient, with the predominance of one or the other being only detectable if RAPtm is measured while tidal volumes are modified. CO: Cardiac output; PAW: Airway pressure; PPL: Pleural pressure; PTP: Transpulmonary pressure; RAP: Right atrial pressure; RPATM: Transmural right atrial pressure; RV: Right ventricle; RVEDP: Right ventricular end-diastolic pressure; RVESP: Right ventricular end-systolic pressure; VR: Venous return; VT: Tidal volume
Comment on
-
Coexistence of a fluid responsive state and venous congestion signals in critically ill patients: a multicenter observational proof-of-concept study.Crit Care. 2024 Feb 19;28(1):52. doi: 10.1186/s13054-024-04834-1. Crit Care. 2024. PMID: 38374167 Free PMC article.
References
-
- Reuter DA, Bayerlein J, Goepfert MSG, Weis FC, Kilger E, Lamm P, et al. Influence of tidal volume on left ventricular stroke volume variation measured by pulse contour analysis in mechanically ventilated patients. Intensive Care Med. 2003;29(3):476–80. - PubMed
-
- Jardin F, Brun-Ney D, Cazaux P, Dubourg O, Hardy A, Bourdarias JP. Relation between transpulmonary pressure and right ventricular isovolumetric pressure change during respiratory support. Cathet Cardiovasc Diagn. 1989;16(4):215–20. - PubMed
-
- Lansdorp B, Hofhuizen C, van Lavieren M, van Swieten H, Lemson J, van Putten MJAM, et al. Mechanical ventilation-induced intrathoracic pressure distribution and heart-lung interactions*. Crit Care Med. 2014;42(9):1983. - PubMed
-
- Mahjoub Y, Pila C, Friggeri A, Zogheib E, Lobjoie E, Tinturier F, et al. Assessing fluid responsiveness in critically ill patients: false-positive pulse pressure variation is detected by Doppler echocardiographic evaluation of the right ventricle. Crit Care Med. 2009;37(9):2570–5. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
