

Effects of the urinary urea excretion index on the decision to wean ICU patients with acute kidney injury from renal replacement therapy: a before-after multicentre study (D-STOP)
- PMID: 40598590
- PMCID: PMC12210492
- DOI: 10.1186/s13054-025-05289-8
Effects of the urinary urea excretion index on the decision to wean ICU patients with acute kidney injury from renal replacement therapy: a before-after multicentre study (D-STOP)
Abstract
Background: The weaning of critical care patients with acute kidney injury (AKI) from renal replacement therapy (RRT) lacks predictive criteria. The urinary urea excretion index (UUEI) based on the urine urea concentration and diuresis may be a relevant prognostic criterion. The aim of this study was to assess the value of utilising a UUEI-based weaning protocol from a RRT catheter.
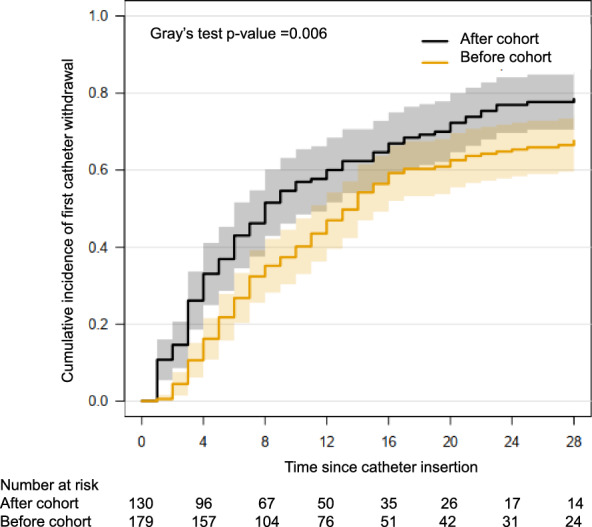
Methods: This was a multicentre before-after study including patients with non-obstructive AKI requiring RRT during their intensive care unit (ICU) stay. A before cohort (2013-2015) was compared to an after cohort (2017-2019) in the interval of which a UUEI-based weaning protocol was implemented. In the after cohort, as soon as the UUEI exceeded 1.35 mmol/kg/24 h, physicians were encouraged to stop RRT and withdraw the catheter, whereas in the before cohort the catheter was withdrawn at the physician's discretion. The primary outcome was the number of RRT catheter-free days on day 28 after initiating RRT.
Results: In total, 179 and 130 patients were included in the before and after cohorts, respectively. The median numbers of catheter-free days in the before and after cohorts on day 28 were 13.0 (IQR 0.0-21.0) vs. 16.5 (IQR 4.3-24.0), respectively (p = 0.02). The adjusted rate ratio for the number of catheter-free days over the number of days at risk was 1.11 (95% CI 1.03-1.19; p = 0.006) in favour of the after cohort. Catheters were reinserted to resume RRT in 3 vs. 5 patients in the before and after cohorts, respectively.
Conclusions: These results confirm that a UUEI-based protocol is a safe technique to prompt withdrawal of the RRT catheter in patients with AKI requiring RRT during their ICU stay.
Trial registration: ClinicalTrials.gov NCT03763188.
Keywords: Acute kidney injury; Intensive care unit; Renal replacement therapy; Urinary urea excretion index.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: The study was approved by the French commission for individual freedom “Commission Nationale des Libertés Individuelles (CNIL)” and the ethic committee of the intensive care unit French society “Société de Réanimation de langue Française (SRLF)”. Consent for publication: All patients accepted their personal data to be registered and used for clinical research purpose. Competing interests: LLG: none CG: none JP: none AM: none CR: none HG: received fees from Baxter, Freseniusnone AR: none AD: received grant support from MSDavenir; fees for conferences symposium from MSD, Pfizer, Novartis, Baxter, Cytosorb, ISep; fees for participation to advisory board from Ocean Dx DG: none RP: none SR; received fees from AstraZeneca, Servier, Novartis, Fresenius, Meditor, Alexion AO: none AB none.
Figures


Comment in
-
Urinary urea excretion index to guide weaning from renal replacement therapy in patients with acute kidney injury: Still haven't found what i'm weaning for.Crit Care. 2025 Jul 26;29(1):326. doi: 10.1186/s13054-025-05581-7. Crit Care. 2025. PMID: 40713649 Free PMC article. No abstract available.
-
From "when to stop" to "why continue today?": operationalizing RRT weaning with UUEI.Crit Care. 2025 Nov 13;29(1):486. doi: 10.1186/s13054-025-05759-z. Crit Care. 2025. PMID: 41233819 Free PMC article. No abstract available.
References
-
- Hoste EAJ, Bagshaw SM, Bellomo R, et al. Epidemiology of acute kidney injury in critically ill patients: the multinational AKI-EPI study. Intensive Care Med. 2015;41:1411–23. 10.1007/s00134-015-3934-7. - PubMed
-
- Gaudry S, Hajage D, Schortgen F, et al. Initiation strategies for renal-replacement therapy in the intensive care unit. N Engl J Med. 2016;375:122–33. 10.1056/NEJMoa1603017. - PubMed
-
- The STARRT-AKI Investigators. Timing of initiation of renal-replacement therapy in acute kidney injury. N Engl J Med. 2020;383:240–51. 10.1056/NEJMoa2000741. - PubMed
-
- Barbar SD, Clere-Jehl R, Bourredjem A, et al. Timing of renal-replacement therapy in patients with acute kidney injury and sepsis. N Engl J Med. 2018;379:1431–42. 10.1056/NEJMoa1803213. - PubMed
-
- Klarenbach S, Manns B, Pannu N, et al. Economic evaluation of continuous renal replacement therapy in acute renal failure. Int J Technol Assess Health Care. 2009;25:331–8. 10.1017/S0266462309990134. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
