

Perisurgical colony stimulating factor one treatment ameliorates liver ischaemia/reperfusion injury in rats
- PMID: 40599188
- PMCID: PMC12207545
- DOI: 10.3748/wjg.v31.i24.108234
Perisurgical colony stimulating factor one treatment ameliorates liver ischaemia/reperfusion injury in rats
Abstract
Background: In the context of hepatobiliary and liver transplant surgery, ischemia-reperfusion (I/R) injury can occur due to temporary interruption of blood flow to the organ followed by a potentially damaging inflammatory response to reperfusion. Macrophages can drive inflammation in response to injury, but they can also promote liver growth and resolution of chronic liver injury and fibrosis. In chronic liver injury models in mice, macrophage colony stimulating factor (CSF)1 stimulates pro-regenerative macrophages.
Aim: To determine whether stimulation of macrophages with macrophage CSF could promote liver repair after I/R injury.
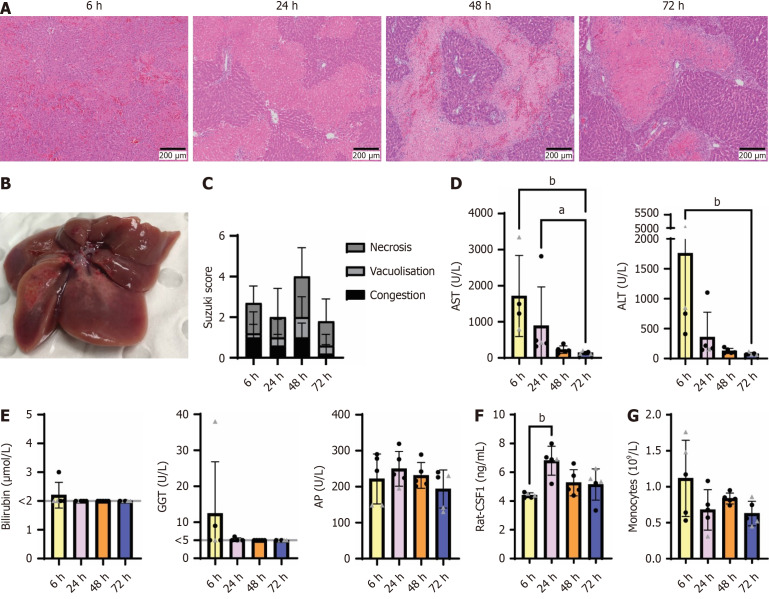
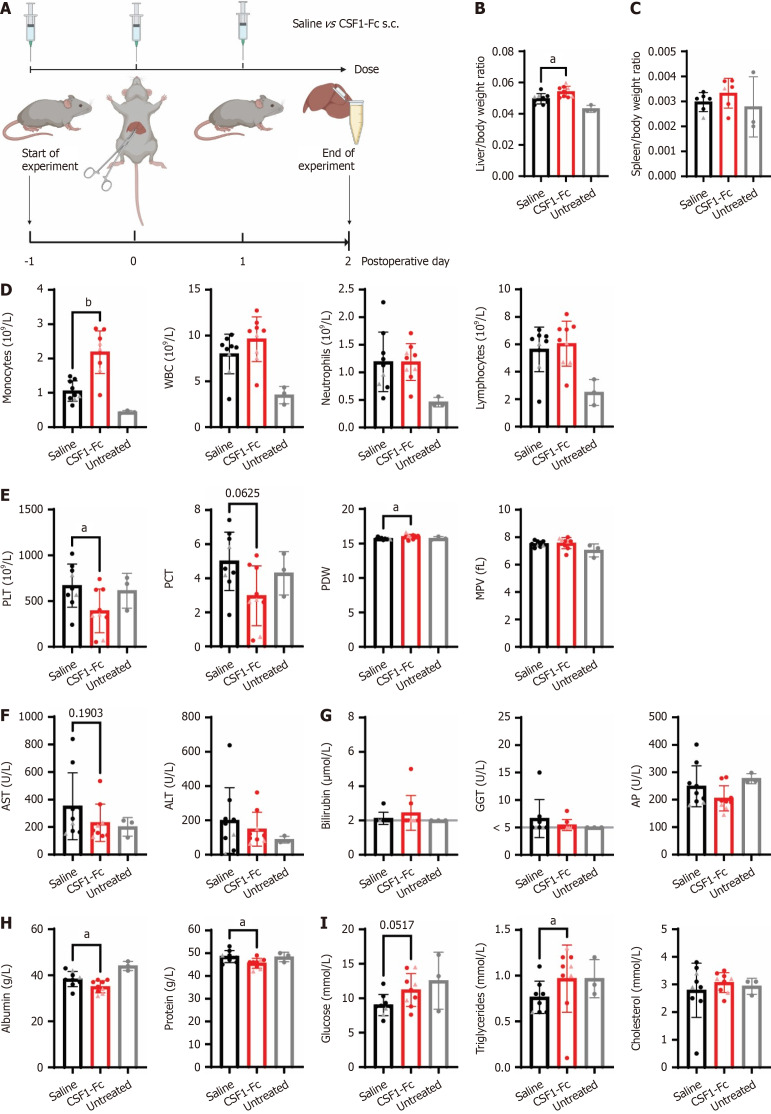
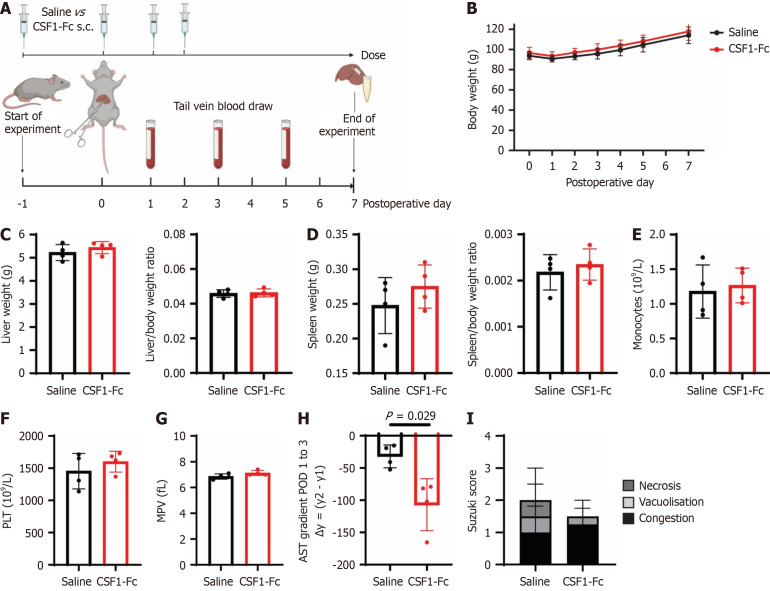
Methods: We investigated the impact of perisurgical treatment with a long-circulating CSF1-Fc conjugate on liver injury and hepatocyte proliferation after 70% ischemia for 60 minutes at 6 hours, 48 hours and 7 days post reperfusion in rats. Circulating and liver tissue monocyte and macrophage subsets in the ischaemic and oxygenated lobes were assessed using quantitative PCR and flow cytometry.
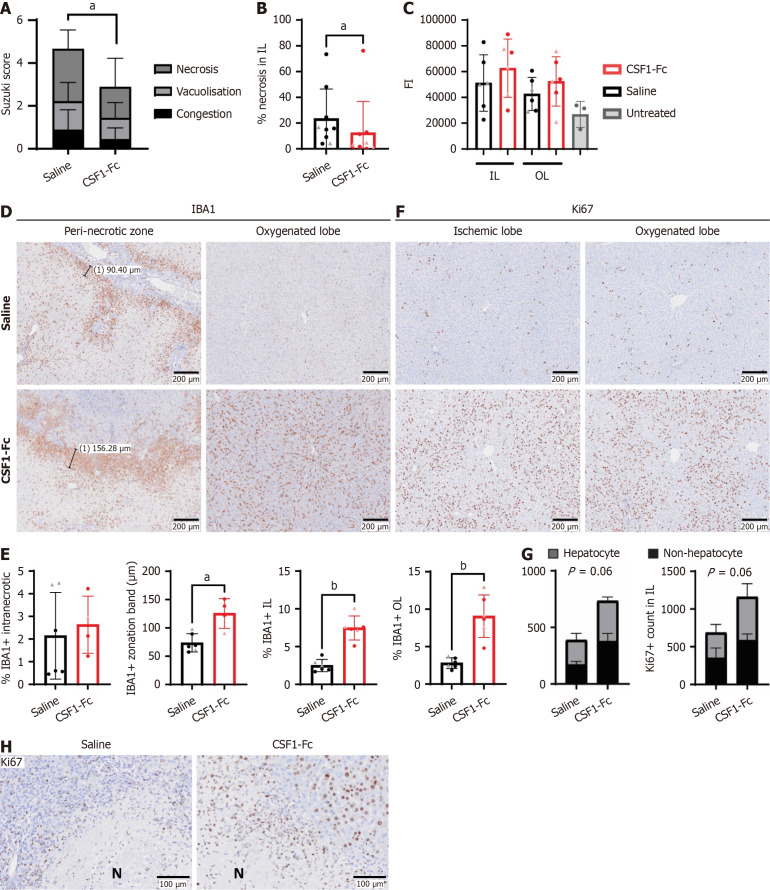
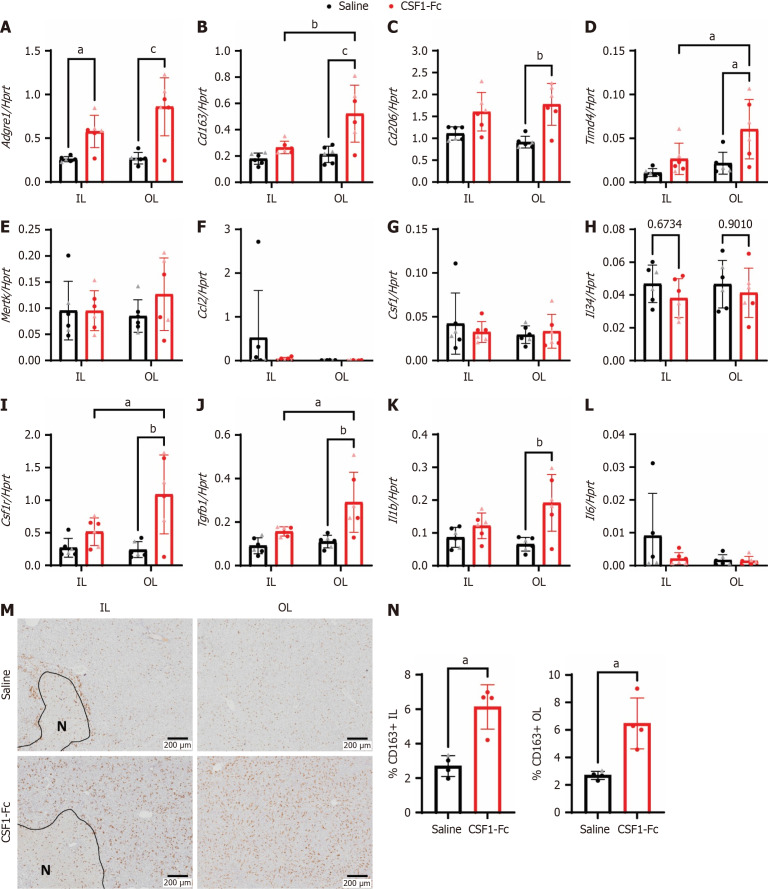
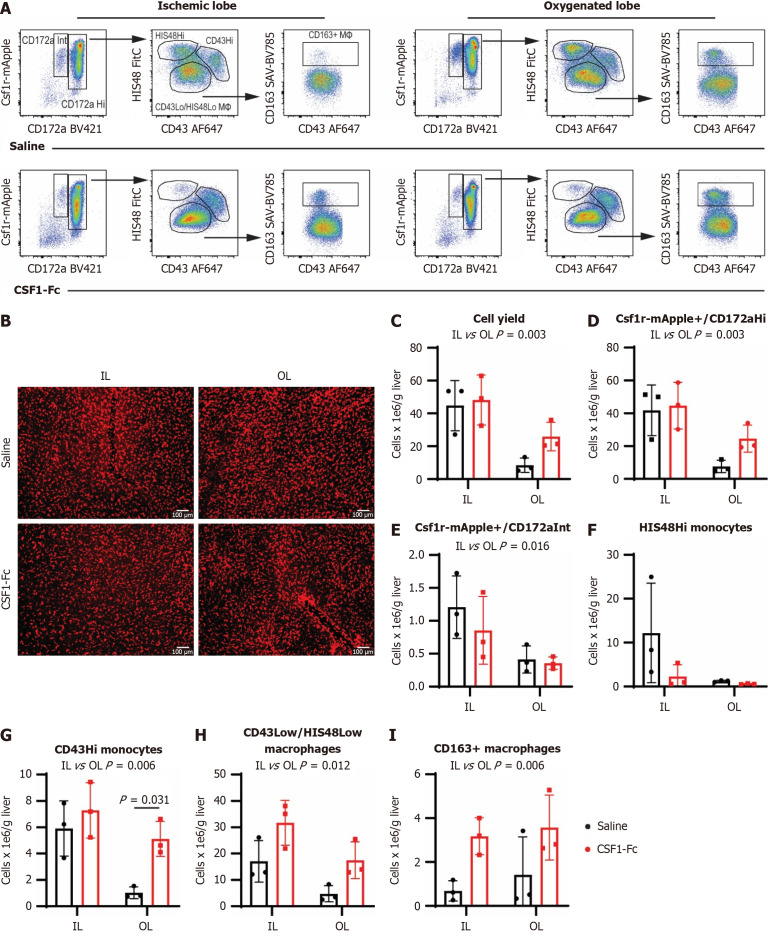
Results: CSF1-Fc treatment did not affect the extent of hepatocellular injury post-reperfusion, as indicated by serum transaminases. Liver I/R injury, especially necrotic area, was reduced in CSF1-Fc-treated rats 48 h post-surgery. This was associated with increased accumulation of macrophages in both the oxygenated and ischemic lobes (ILs), and peri-necrotic zone localization in the IL. CSF1-Fc treatment also promoted liver growth, associated with increased parenchymal and non-parenchymal cell proliferation. CSF1-Fc increased the abundance of CD43+ non-classical monocytes, consistent with the role of CSF1 signaling in monocyte maturation, and increased CD163 expression on mature macrophages.
Conclusion: This study suggests CSF1 stimulation drives monocytes/macrophages towards a pro-regenerative response and perisurgical CSF1 treatment might augment liver regeneration in patients undergoing liver resection.
Keywords: Hepatectomy; Innate immunity; Ischaemia; Liver; Macrophages; Necrosis; Regeneration.
©The Author(s) 2025. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Ischaemic preconditioning for the reduction of renal ischaemia reperfusion injury.Cochrane Database Syst Rev. 2017 Mar 4;3(3):CD010777. doi: 10.1002/14651858.CD010777.pub2. Cochrane Database Syst Rev. 2017. PMID: 28258686 Free PMC article.
-
HuR inhibition reduces post-ischemic cardiac remodeling by dampening myocyte-dependent inflammatory gene expression and the innate immune response.FASEB J. 2025 Mar 31;39(6):e70433. doi: 10.1096/fj.202400532RRR. FASEB J. 2025. PMID: 40085190 Free PMC article.
-
Alamandine: Protective Effects Against Renal Ischemia-Reperfusion Injury-Induced Renal and Liver Damage in Diabetic Rats.J Biochem Mol Toxicol. 2025 Aug;39(8):e70423. doi: 10.1002/jbt.70423. J Biochem Mol Toxicol. 2025. PMID: 40741878
-
Pharmacological interventions for ischaemia reperfusion injury in liver resection surgery performed under vascular control.Cochrane Database Syst Rev. 2009 Oct 7;2009(4):CD008154. doi: 10.1002/14651858.CD008154. Cochrane Database Syst Rev. 2009. PMID: 19821445 Free PMC article.
-
Granulocyte colony-stimulating factor with or without stem or progenitor cell or growth factors infusion for people with compensated or decompensated advanced chronic liver disease.Cochrane Database Syst Rev. 2023 Jun 6;6(6):CD013532. doi: 10.1002/14651858.CD013532.pub2. Cochrane Database Syst Rev. 2023. PMID: 37278488 Free PMC article.
References
-
- Ishizaki Y, Yoshimoto J, Miwa K, Sugo H, Kawasaki S. Safety of prolonged intermittent pringle maneuver during hepatic resection. Arch Surg. 2006;141:649–53; discussion 654. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
