

Quality of Life After Mitral Transcatheter Edge-to-Edge Repair According to Baseline Tricuspid Regurgitation
- PMID: 40599385
- PMCID: PMC12207239
- DOI: 10.1016/j.shj.2024.100408
Quality of Life After Mitral Transcatheter Edge-to-Edge Repair According to Baseline Tricuspid Regurgitation
Abstract
Background: There is a high prevalence of significant tricuspid regurgitation (TR) in patients undergoing mitral transcatheter edge-to-edge repair (M-TEER). Significant TR is associated with poor prognosis and affects decision-making between M-TEER and concomitant mitral and tricuspid valve surgery. Improved quality of life (QoL) is an important metric for patients.
Methods: We analyzed data from 1838 patients undergoing M-TEER included in a multicenter statewide registry from 2015 to 2023. QoL was assessed using baseline and 30-day Kansas City Cardiomyopathy Questionnaire (KCCQ) scores. Patients were classified as no/mild TR or moderate/severe TR, and changes in KCCQ scores were compared. The primary outcome was an adjusted analysis consisting of survival to 30 days with a ≥15-point improvement in KCCQ score.
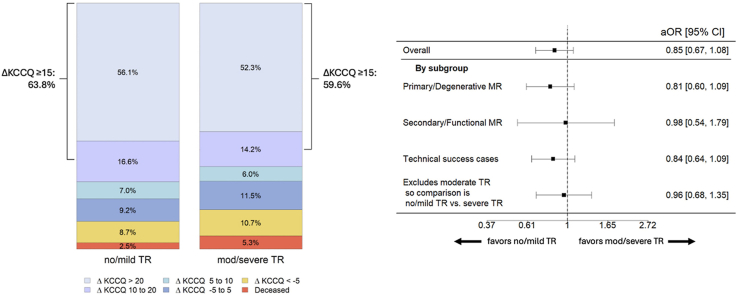
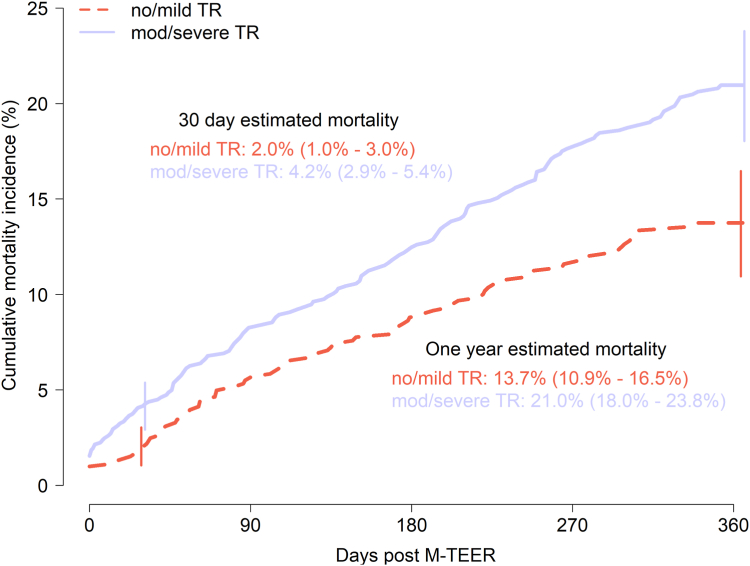
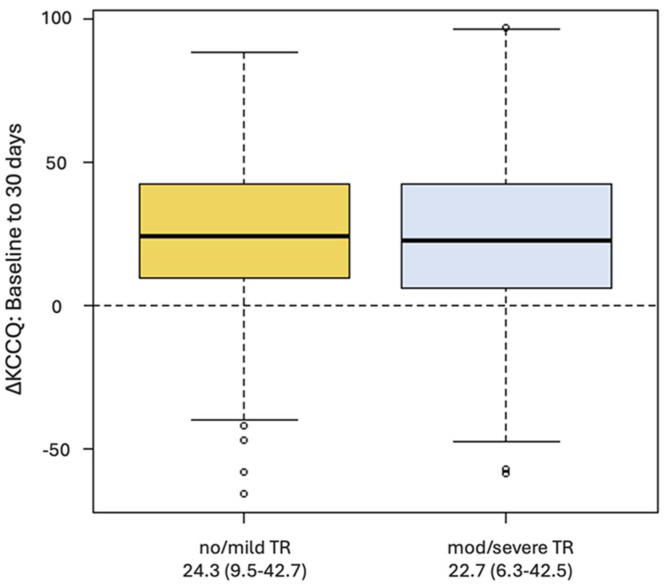
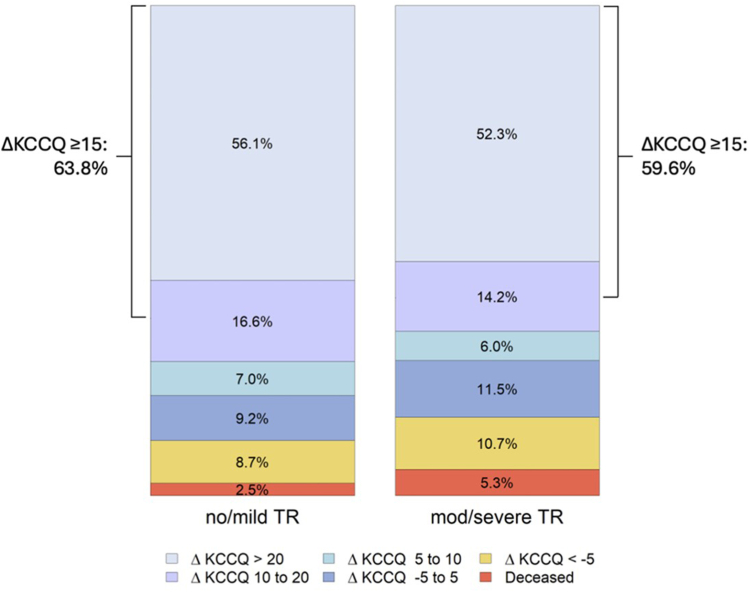
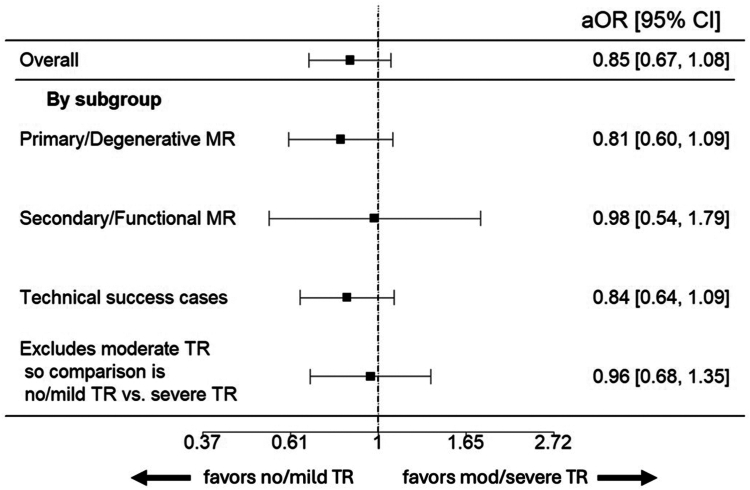
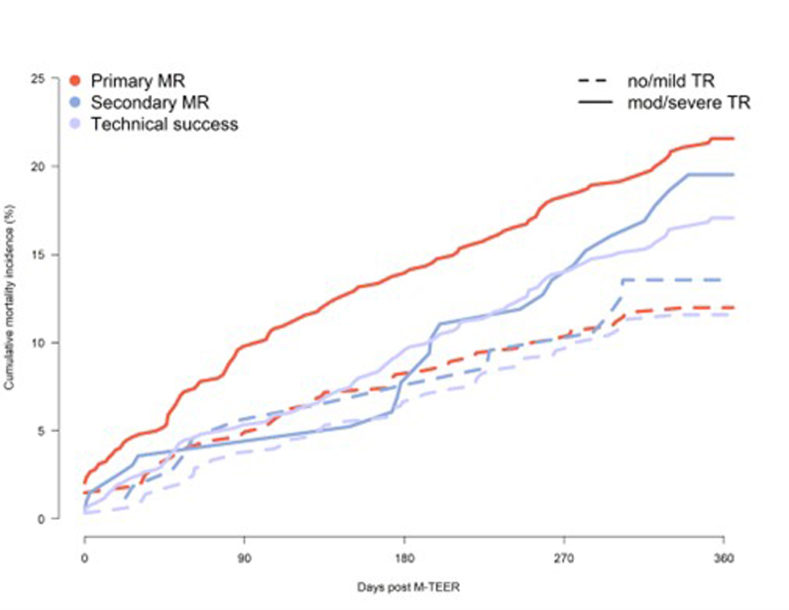
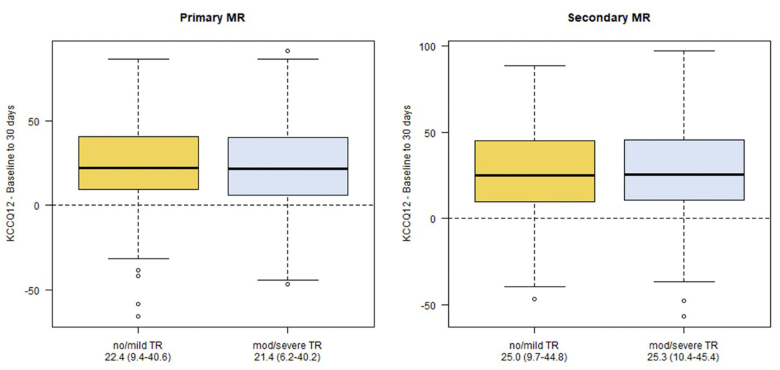
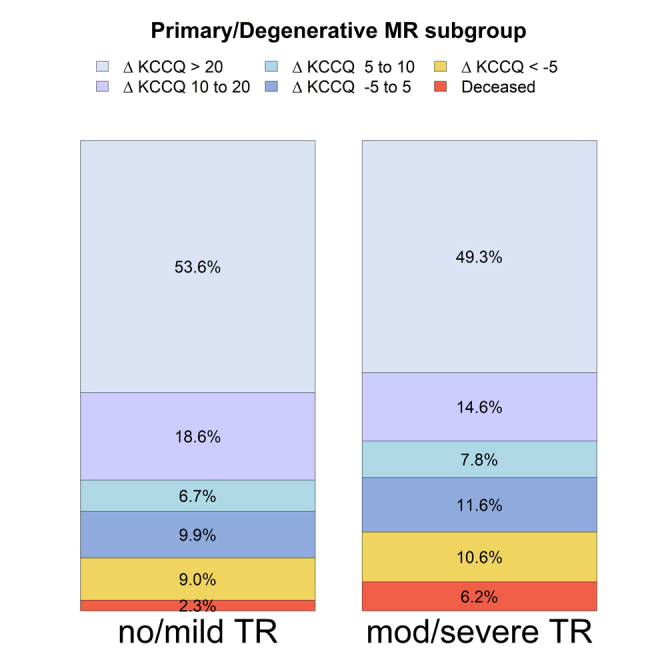
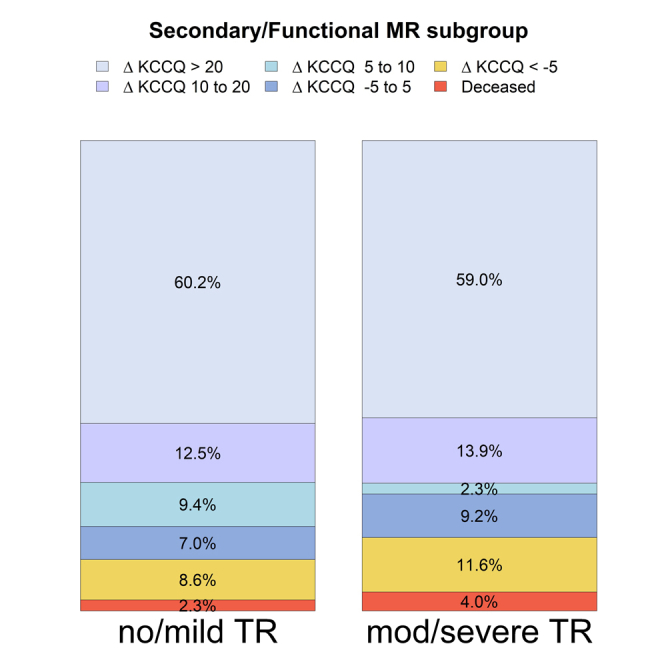
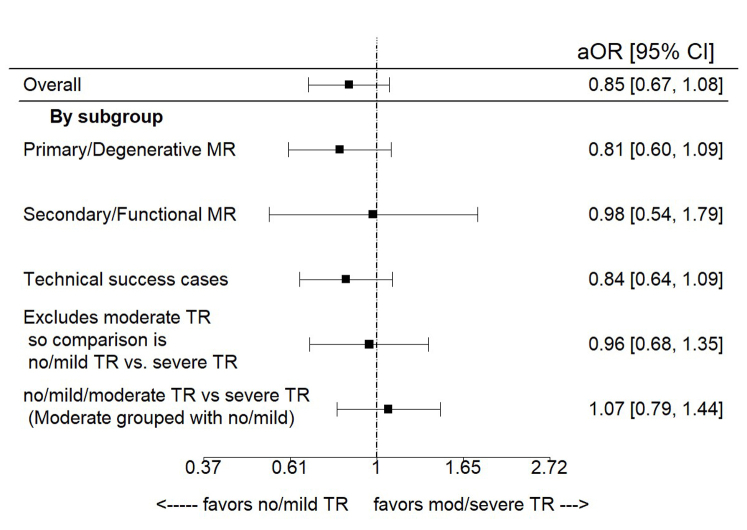
Results: Complete endpoint data were available for 1421 patients (77.3%). On average, patients undergoing M-TEER experienced large improvements in QoL, regardless of baseline TR group. Thirty-day mortality for patients with moderate/severe TR was higher than for those with no/mild TR (42 [4.1%] vs. 16 [2.0%], respectively, p = 0.018). The majority of patients survived to 30 days with ΔKCCQ ≥15 (63.8% for no/mild TR vs. 59.6% for moderate/severe TR, p = 0.120). Patients with moderate/severe TR exhibited no difference in the primary adjusted outcome (adjusted odds ratio: 0.851, p = 0.177).
Conclusions: The majority of patients experience a large improvement in QoL after M-TEER, regardless of baseline TR severity. Further research should explore a staged approach of M-TEER followed by tricuspid valve intervention as needed compared to concomitant mitral/tricuspid valve surgery.
Keywords: Health-related quality of life (QoL); Mitral regurgitation (MR); Mitral transcatheter edge-to-edge repair (M-TEER); Tricuspid regurgitation (TR); Tricuspid transcatheter edge-to-edge repair (T-TEER).
Figures
References
-
- Sagie A., Freitas N., Chen M.H., Marshall J.E., Weyman A.K., Levine R.A. Echocardiographic assessment of mitral stenosis and its associated valvular lesions in 205 patients and lack of association with mitral valve prolapse. J Am Soc Echocardiogr. 1997;10(2):141–148. doi: 10.1016/S0894-7317(97)70086-5. - DOI - PubMed
LinkOut - more resources
Full Text Sources
