

Recurrent Clostridioides difficile Infection (CDI) in Patients Treated With Vancomycin at Johns Hopkins Aramco Healthcare (JHAH), Dhahran, Saudi Arabia
- PMID: 40599506
- PMCID: PMC12208806
- DOI: 10.7759/cureus.85116
Recurrent Clostridioides difficile Infection (CDI) in Patients Treated With Vancomycin at Johns Hopkins Aramco Healthcare (JHAH), Dhahran, Saudi Arabia
Abstract
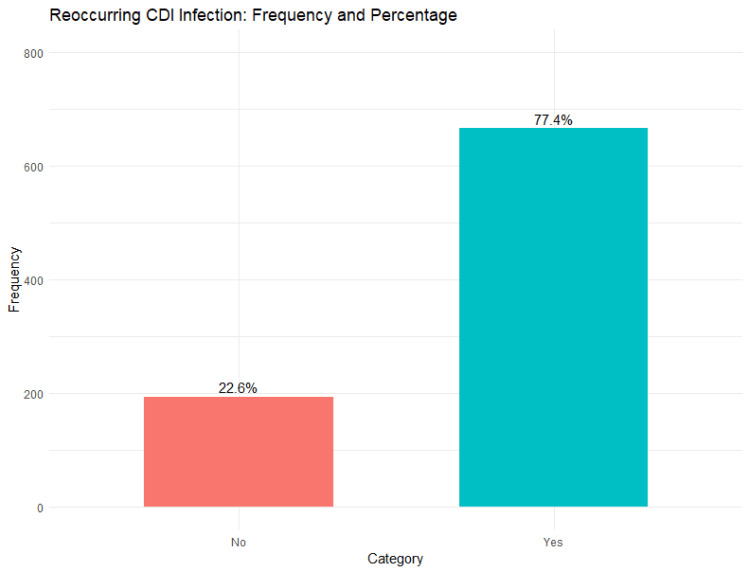
Introduction Clostridioides difficile infection (CDI) is a leading cause of healthcare-associated diarrhea with a significant risk of recurrence, posing challenges for patient management and infection control. Identifying risk factors for recurrence is essential to improve outcomes and prevent relapses. Methods This retrospective cohort study included 860 adult patients (≥18 years) treated with vancomycin for CDI at Johns Hopkins Aramco Healthcare (JHAH) in Dhahran, Saudi Arabia, between January 2015 and December 2020. Patients with confirmed CDI based on stool polymerase chain reaction (PCR) or toxin assays, complete medical records, and adequate follow-up data were included. The study excluded those not treated with vancomycin, under 18 years of age, with incomplete records, those who received fecal microbiota transplantation or experimental treatments, and those lacking follow-up data. Data on demographics, comorbidities, hospitalization, medication use, and recurrence were analyzed using univariate and multivariate logistic regression models. Results Univariate analysis showed that age 40-65 years (OR = 1.53; 95% CI: 1.024-2.285; p = 0.038), age >65 years (OR = 1.894; 95% CI: 1.282-2.799; p = 0.001), cirrhosis (OR = 9.104; 95% CI: 1.233-67.192; p = 0.03), hospitalization (OR = 1.974; 95% CI: 1.417-2.749; p < 0.0001), and type 2 diabetes mellitus (OR = 1.65; 95% CI: 1.106-2.462; p = 0.014) were significantly associated with CDI recurrence. After adjusting for confounders, only hospitalization remained a statistically significant independent predictor (OR = 1.597; 95% CI: 1.098-2.325; p = 0.014). Conclusion Hospitalization was identified as the most significant independent risk factor for CDI recurrence. These findings highlight the need for enhanced infection control practices and close monitoring of hospitalized patients with CDI. Future prospective and multicenter studies are recommended to validate these results and explore additional modifiable risk factors to reduce recurrence rates.
Keywords: clostridioides difficile recurrence rate; clostridium difficile; clostridium difficile treatment; dhahran; johns hopkins aramco healthcare; recurrent clostridioides difficile infection; saudi arabia; vancomycin; vancomycin treatment.
Copyright © 2025, Alnahwi et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Johns Hopkins Aramco Healthcare (JHAH) Institutional Review Board (IRB) issued approval H-05-DH-044. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Fecal microbiota transplantation for the treatment of recurrent Clostridioides difficile (Clostridium difficile).Cochrane Database Syst Rev. 2023 Apr 25;4(4):CD013871. doi: 10.1002/14651858.CD013871.pub2. Cochrane Database Syst Rev. 2023. PMID: 37096495 Free PMC article.
-
Antibiotic treatment for Clostridium difficile-associated diarrhoea in adults.Cochrane Database Syst Rev. 2017 Mar 3;3(3):CD004610. doi: 10.1002/14651858.CD004610.pub5. Cochrane Database Syst Rev. 2017. PMID: 28257555 Free PMC article.
-
Antibiotic treatment for Clostridium difficile-associated diarrhea in adults.Cochrane Database Syst Rev. 2011 Sep 7;(9):CD004610. doi: 10.1002/14651858.CD004610.pub4. Cochrane Database Syst Rev. 2011. Update in: Cochrane Database Syst Rev. 2017 Mar 03;3:CD004610. doi: 10.1002/14651858.CD004610.pub5. PMID: 21901692 Updated.
-
Real-world use of bezlotoxumab to prevent recurrent Clostridioides difficile infections: a single-center experience and meta-analysis.Therap Adv Gastroenterol. 2025 Jun 21;18:17562848251346593. doi: 10.1177/17562848251346593. eCollection 2025. Therap Adv Gastroenterol. 2025. PMID: 40547251 Free PMC article.
-
Antibiotic treatment for Clostridium difficile-associated diarrhea in adults.Cochrane Database Syst Rev. 2005 Jan 25;(1):CD004610. doi: 10.1002/14651858.CD004610.pub2. Cochrane Database Syst Rev. 2005. Update in: Cochrane Database Syst Rev. 2007 Jul 18;(3):CD004610. doi: 10.1002/14651858.CD004610.pub3. PMID: 15674956 Updated.
References
-
- Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA) McDonald LC, Gerding DN, Johnson S, et al. Clin Infect Dis. 2018;66:0–48. - PMC - PubMed
LinkOut - more resources
Full Text Sources