

Incidence of cardiovascular risk factors and exercise phenotyping in cardiomyopathies: One size does not fit all
- PMID: 40599641
- PMCID: PMC12210320
- DOI: 10.1016/j.ijcha.2025.101722
Incidence of cardiovascular risk factors and exercise phenotyping in cardiomyopathies: One size does not fit all
Abstract
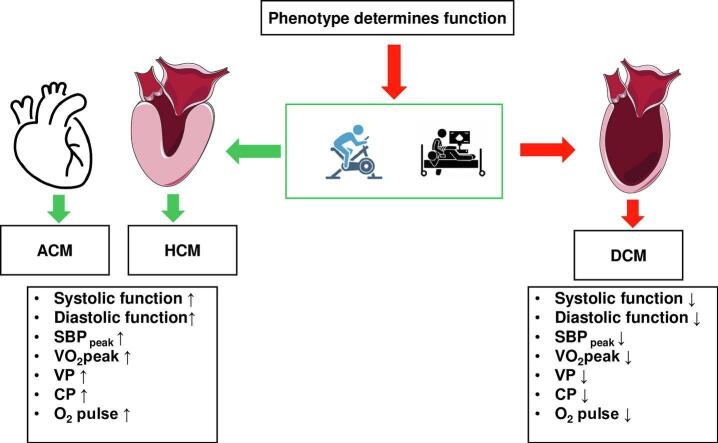
Background: Cardiovascular disease risk factors (CVDRF) are linked to increased morbidity in cardiomyopathies (CMP), but whether new onset CVDRF differ among CMPs is unknown. In addition, whether the acute exercise response during cardiopulmonary exercise testing (CPET) differs among CMPs remains unclear.
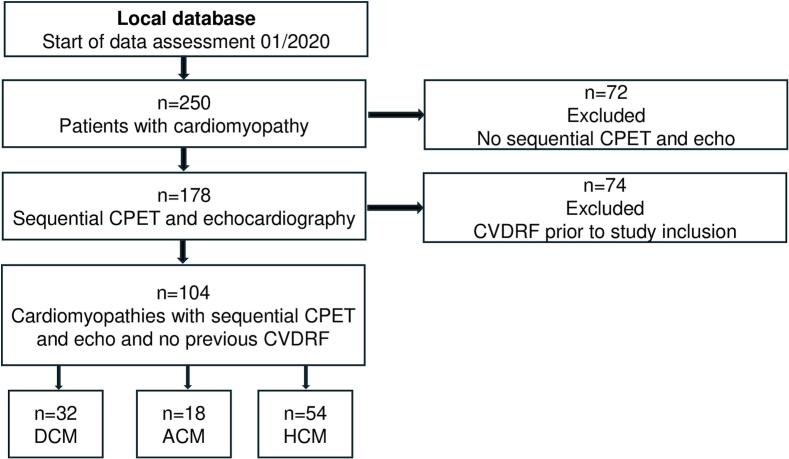
Methods: This single-center, retrospective study analyzed patients with arrhythmogenic, hypertrophic, and dilated (DCM) cardiomyopathy without CVDRF at baseline. Resting echocardiography and CPET were performed, and exercise response was assessed depending on sex and CMP. After a median follow-up of 19.5 months, CPET and echocardiography were analyzed in relation to the development of new CVDRF.
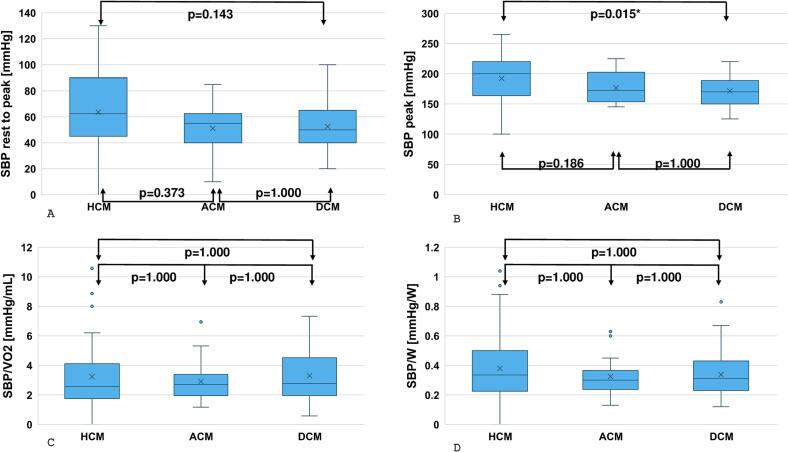
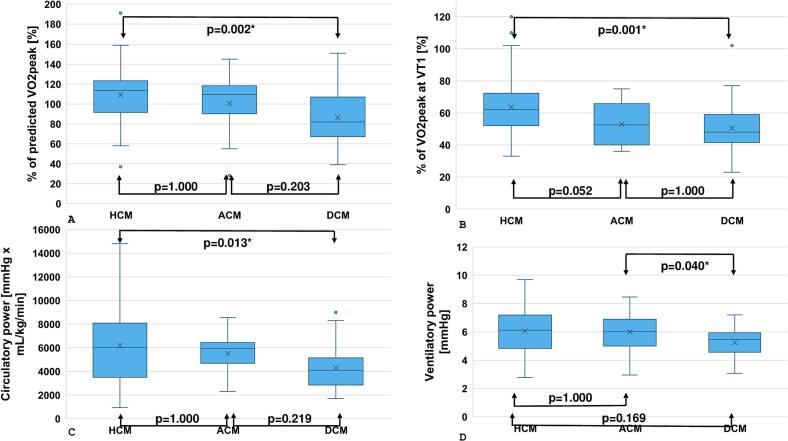
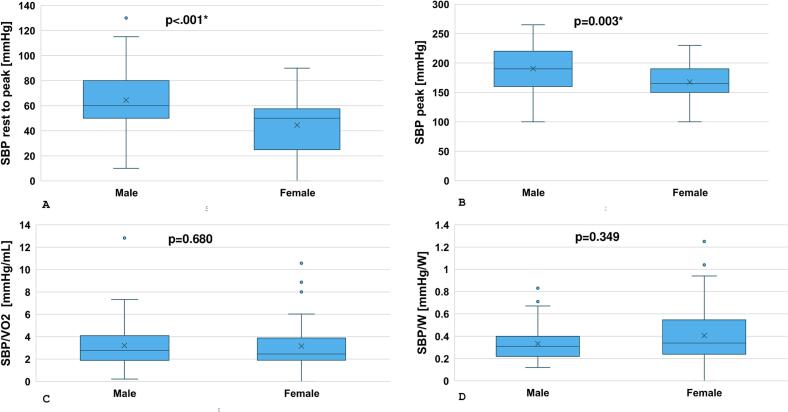
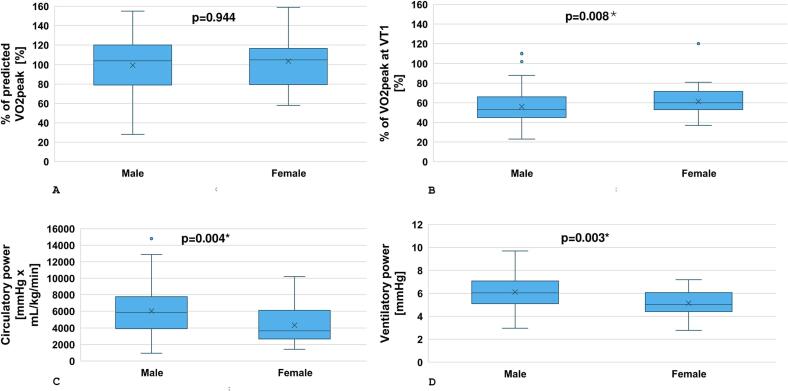
Results: A total of 104 CMPs were included (median age 53.0 years). New-onset CVDRF was rare (11.5 %) and driven by arterial hypertension (8.7 %) but did not differ among CMPs. DCM displayed significantly lower resting left ventricular ejection fraction (40.5 %, interquartile range, IQR, 11.5 %, p < 0.001), diastolic function (E/e' 9.3, IQR 5.5, p < 0.001), and had the lowest peak systolic blood pressure (170.0 mmHg, IQR 52.5 mmHg, p = 0.011), predicted peak oxygen consumption (82.0 %, IQR 39.8 %, p = 0.003), oxygen pulse (101.0 %, IQR 28.8 %, p = 0.030) as well as lower ventilatory (VP, 5.5 mmHg, IQR 1.4 mmHg, p = 0.033) and circulatory (CP, 4096.0 mL/kg/min x mmHg, IQR 2299.3 mL/kg/min x mmHg, p = 0.015) power compared to the other groups. Lower VP (5.0 mmHg, IQR 1.3 mmHg, p = 0.003) and CP (3660.0 mL/kg/min x mmHg, IQR 3298.0 mL/kg/min x mmHg, p = 0.004) were observed for females.
Conclusions: Arterial hypertension was the most common CVDRF among CMPs, underscoring the importance of monitoring this outcome. Exercise limitations differ between CMPs and should be interpreted depending on sex.
Keywords: Cardiomyopathy; Cardiovascular risk factors; Circulatory limitations; Exercise blood pressure.
© 2025 The Author(s).
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: [SW has received honoraria for lectures from Bristol-Myers Squibb. MHay is funded, in part, by a Research Chair in Aging in the Faculty of Nursing, College of Healthy Sciences at UofA. MH reports honoraria for lectures from Abbott, Amgen, Astra- Zeneca, Boehringer-Ingelheim, BMW, Bristol-Myers Squibb, Daiichi-Sankyo, Lilly, Medi, MSD Sharp & Dohme GmbH, Norsan, Novartis, Pfizer and Roche, consulting fees from Medical Park. No other potential conflicts of interest are reported.].
Figures
References
-
- Arbelo E., Protonotarios A., Gimeno J.R., Arbustini E., Barriales-Villa R., Basso C., et al. 2023 ESC guidelines for the management of cardiomyopathies. Eur. Heart J. 2023;44:3503–3626. - PubMed
-
- Ommen S.R., Ho C.Y., Asif I.M., Balaji S., Burke M.A., Day S.M., et al. 2024 AHA/ACC/AMSSM/HRS/PACES/SCMR guideline for the Management of Hypertrophic Cardiomyopathy: a report of the American Heart Association/American College of Cardiology Joint Committee on clinical Practice guidelines. Circulation. 2024;149:e1239–e1311. - PubMed
-
- Guazzi M., Wilhelm M., Halle M., Van Craenenbroeck E., Kemps H., de Boer R.A., et al. Exercise testing in heart failure with preserved ejection fraction: an appraisal through diagnosis, pathophysiology and therapy - A clinical consensus statement of the Heart failure association and European Association of Preventive Cardiology of the European Society of Cardiology. Eur. J. Heart Fail. 2022;24:1327–1345. - PMC - PubMed
-
- Ribeiro G.D.S., Deresz L.F., Salvioni E., Hansen D., Agostoni P., Karsten M. Sensitivity and specificity of different exercise oscillatory ventilation definitions to predict 2-year major adverse cardiovascular outcomes in chronic heart failure patients. Int. J. Cardiol. 2022;360:39–43. - PubMed
-
- Buber J., Robertson H.T. Cardiopulmonary exercise testing for heart failure: pathophysiology and predictive markers. Heart. 2023;109:256–263. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
