

Mesenchymal stem cell therapy for breast cancer-related secondary lymphedema (Review)
- PMID: 40599719
- PMCID: PMC12210111
- DOI: 10.3892/mco.2025.2868
Mesenchymal stem cell therapy for breast cancer-related secondary lymphedema (Review)
Abstract
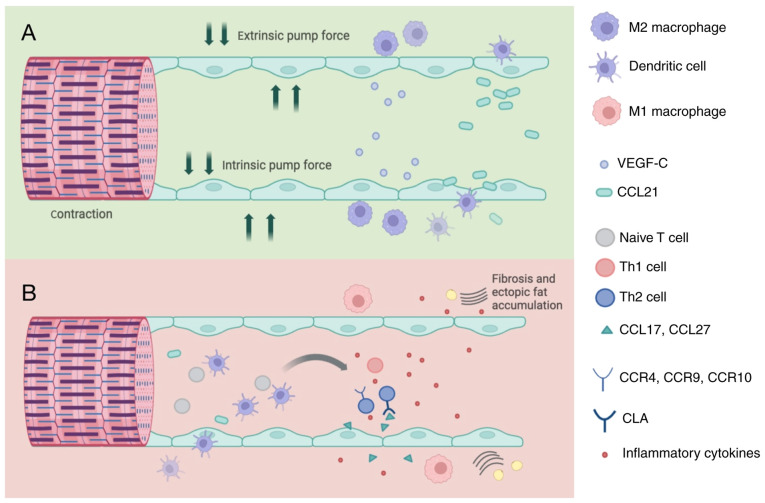
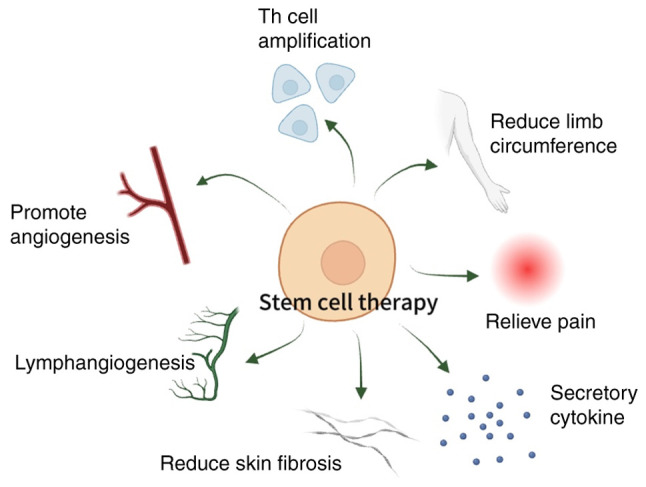
Secondary lymphedema, affecting ~15-30% of patients who survive breast cancer, is a common consequence following treatment. At present, there is no gold standard for the treatment of breast cancer-related lymphedema (BCRL). Conventional methods such as physiotherapy and surgery demonstrate a limited effectiveness in mitigating lymphatic swelling or discomfort and fail to provide substantial physiological improvement or a definitive cure for lymphedema. However, stem cell therapy has garnered notable attention due to its regenerative potential and its capacity to modulate inflammatory processes. Mesenchymal stem cell (MSC) therapies exhibit promise in ameliorating BCRL by addressing edema, promoting lymphangiogenesis and mitigating fibrosis. It is shown that MSC therapy promotes the regeneration of autologous lymphatic networks and improves vascular conditions in rodent tail and hindlimb lymphedema models, which offers relief from lymphedema symptoms including limb volume asymmetry and impaired lymphatic drainage. However, currently, due to a lack of a universally recognized or standardized treatment regimen for BCRL, there is a need for additional clinical studies featuring larger sample sizes and extended follow-up periods to further investigate this prospective therapeutic modality. The present review aims to provide guidance for further research and therapeutic interventions following the results observed in both preclinical and clinical settings. The present study investigated the pathogenesis of secondary lymphedema, previous advancements in stem cell therapy for this condition and an analysis of persisting challenges.
Keywords: BCRL; MSCs; lymphangiography; regulatory T cells.
Copyright: © 2025 Han et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Herbal and dietary therapies for primary and secondary dysmenorrhoea.Cochrane Database Syst Rev. 2001;(3):CD002124. doi: 10.1002/14651858.CD002124. Cochrane Database Syst Rev. 2001. Update in: Cochrane Database Syst Rev. 2016 Mar 22;3:CD002124. doi: 10.1002/14651858.CD002124.pub2. PMID: 11687013 Updated.
-
Inhaled mannitol for cystic fibrosis.Cochrane Database Syst Rev. 2018 Feb 9;2(2):CD008649. doi: 10.1002/14651858.CD008649.pub3. Cochrane Database Syst Rev. 2018. Update in: Cochrane Database Syst Rev. 2020 May 1;5:CD008649. doi: 10.1002/14651858.CD008649.pub4. PMID: 29424930 Free PMC article. Updated.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of topotecan for ovarian cancer.Health Technol Assess. 2001;5(28):1-110. doi: 10.3310/hta5280. Health Technol Assess. 2001. PMID: 11701100
-
Interventions for acute otitis externa.Cochrane Database Syst Rev. 2010 Jan 20;(1):CD004740. doi: 10.1002/14651858.CD004740.pub2. Cochrane Database Syst Rev. 2010. PMID: 20091565
-
LymphSens study: the enigma of subjective lymphoedema - how often and why do patients report lymphoedema after breast cancer treatment without an objective measurable swelling? The role of lymphatic and sensory processing problems: a protocol for a multicentre prospective longitudinal study.BMJ Open. 2025 Jun 8;15(6):e099990. doi: 10.1136/bmjopen-2025-099990. BMJ Open. 2025. PMID: 40484423 Free PMC article.
References
-
- Aguilera-Eguía RA, Seron P, Gutiérrez-Arias R, Zaror C. Which physical therapy intervention is most effective in reducing secondary lymphoedema associated with breast cancer? Protocol for a systematic review and network meta-analysis. BMJ Open. 2022;12(e065045) doi: 10.1136/bmjopen-2022-065045. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources