

Effect of early neuroendovascular team involvement in acute stroke protocol: a retrospective study
- PMID: 40599733
- PMCID: PMC12209294
- DOI: 10.3389/fneur.2025.1568572
Effect of early neuroendovascular team involvement in acute stroke protocol: a retrospective study
Abstract
Introduction: Acute ischemic stroke (AIS) is a leading cause of morbidity and mortality, with outcomes dependent on timely treatment. Tissue plasminogen activator (tPA) and endovascular therapy (EVT) improve outcomes, but delays reduce their efficacy. This study introduced a protocol featuring early participation of neuroendovascular interventionists and evaluated its association with treatment times and outcomes compared with conventional management.
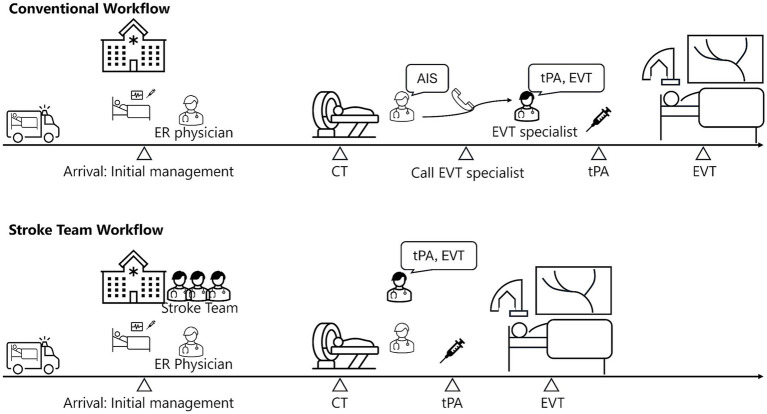
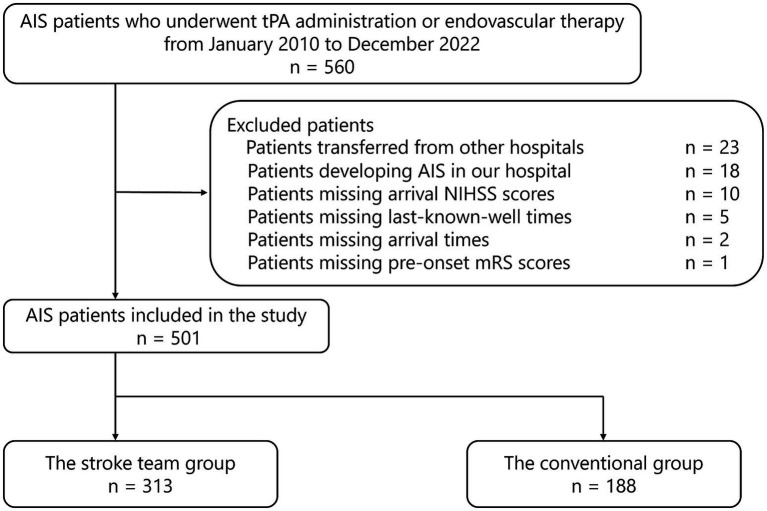
Methods: This single-center retrospective study included patients with AIS transported to emergency room (ER) who received tPA or EVT between January 2010 and December 2022. Under the protocol, the stroke team-including neuroendovascular interventionists, who made the final decision on tPA and EVT-was activated by the emergency physician when stroke was suspected based on pre-hospital information. The stroke team was not activated if neuroendovascular interventionists were engaged in other procedures or if the ER physician suspected a non-stroke diagnosis. Upon arrival, the team commenced care, with neuroendovascular interventionists reviewing imaging and determining treatment strategies. Patients were categorized into protocol and conventional groups based on management under the new protocol or standard care. The primary outcome was a favorable neurological outcome, defined as a modified Rankin Scale (mRS) score of 0-2 at discharge. Secondary outcomes included time metrics for initiation of tPA and/or EVT. Logistic regression analysis estimated the effects of the protocol, adjusting for confounders, including age, sex, baseline National Institutes of Health Stroke Scale score, and pre-hospital factors. Secondary outcomes were assessed using multiple linear regression.
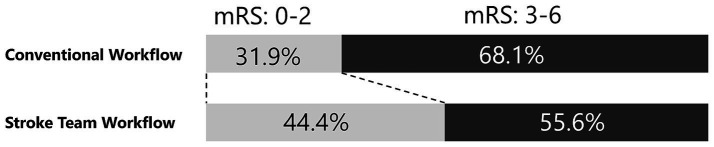
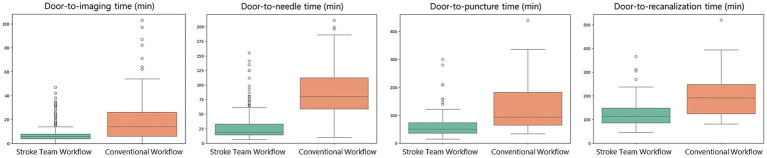
Results: This study analyzed 501 patients, with 313 in the protocol group and 188 in the conventional group. Favorable neurological outcomes at discharge (mRS 0-2) were more frequent in the protocol group (44.4% vs. 31.9%; adjusted odds ratio: 2.92, 95% confidence interval [CI]: 1.83-4.66). The protocol group also showed shorter door-to-imaging time (-8.3 min), door-to-needle time (-55.9 min), door-to-puncture time (-59.8 min), and door-to-recanalization time (-73.7 min).
Conclusion: Early engagement of neuroendovascular specialists in the emergency pathway was associated with faster treatment initiation and a higher likelihood of favorable functional status at discharge in this retrospective cohort. Because residual confounding and temporal changes in stroke care cannot be excluded, prospective validation in other settings is warranted.
Keywords: door-to-treatment time; endovascular therapy; neurological outcomes; stroke team protocol; tissue plasminogen activator; workflow optimization.
Copyright © 2025 Mori, Kashiura, Suzuki, Ono, Yoshimura and Moriya.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Does Augmenting Irradiated Autografts With Free Vascularized Fibula Graft in Patients With Bone Loss From a Malignant Tumor Achieve Union, Function, and Complication Rate Comparably to Patients Without Bone Loss and Augmentation When Reconstructing Intercalary Resections in the Lower Extremity?Clin Orthop Relat Res. 2025 Jun 26. doi: 10.1097/CORR.0000000000003599. Online ahead of print. Clin Orthop Relat Res. 2025. PMID: 40569278
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Thrombolysis for acute ischaemic stroke.Cochrane Database Syst Rev. 2003;(3):CD000213. doi: 10.1002/14651858.CD000213. Cochrane Database Syst Rev. 2003. Update in: Cochrane Database Syst Rev. 2009 Oct 07;(4):CD000213. doi: 10.1002/14651858.CD000213.pub2. PMID: 12917889 Updated.
-
Impact of Off-Hour Admission on In-Hospital Outcomes for Patients With Stroke Receiving Reperfusion Therapy in China.Stroke. 2024 May;55(5):1359-1369. doi: 10.1161/STROKEAHA.123.046096. Epub 2024 Mar 28. Stroke. 2024. PMID: 38545773
-
Home treatment for mental health problems: a systematic review.Health Technol Assess. 2001;5(15):1-139. doi: 10.3310/hta5150. Health Technol Assess. 2001. PMID: 11532236
References
-
- Emberson J, Lees KR, Lyden P, Blackwell L, Albers G, Bluhmki E, et al. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: a meta-analysis of individual patient data from randomised trials. Lancet. (2014) 384:1929–35. doi: 10.1016/S0140-6736(14)60584-5, PMID: - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources