

Self-limited, sodium-dependent osmotic diuresis causes polyuria after living donor kidney transplantation
- PMID: 40599822
- PMCID: PMC12209782
- DOI: 10.1093/ckj/sfaf099
Self-limited, sodium-dependent osmotic diuresis causes polyuria after living donor kidney transplantation
Abstract
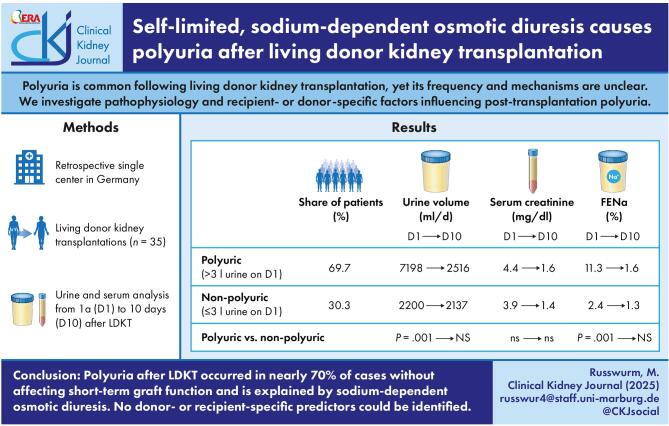
Background and hypothesis: Polyuria, defined as urine output exceeding 3 l per day, is common following living donor kidney transplantation, yet its frequency and mechanisms are unclear. This study investigates the pathophysiology and potential recipient- or donor-specific factors influencing post-transplantation polyuria.
Methods: We retrospectively evaluated 35 consecutive living donor kidney transplantations performed at the University Medical Center Marburg between 2018 and 2024. Clinical and laboratory characteristics of recipients and donors as well as the daily routine blood tests and 24-hour urine collections of the first 10 days post-transplantation were analyzed.
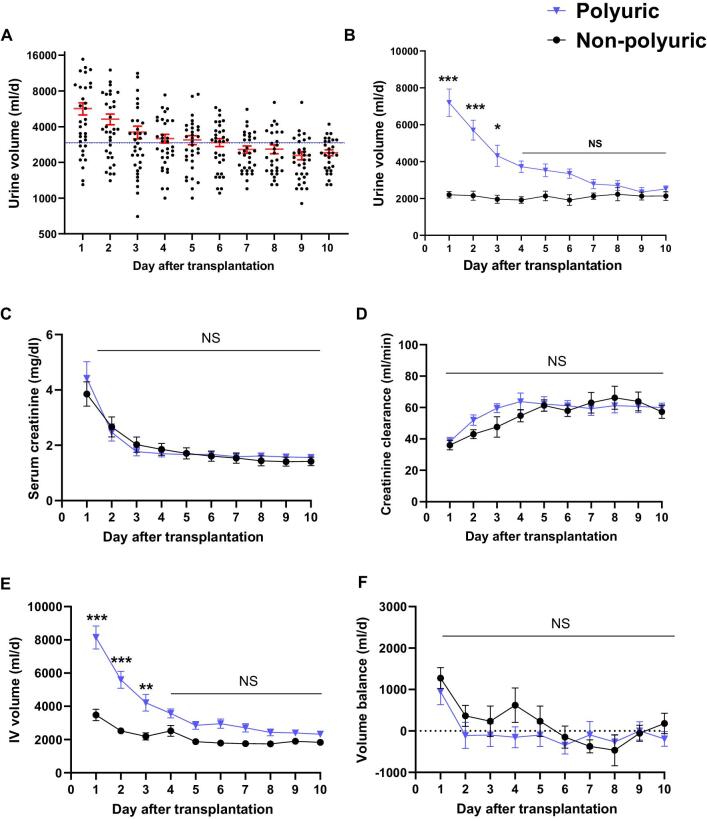
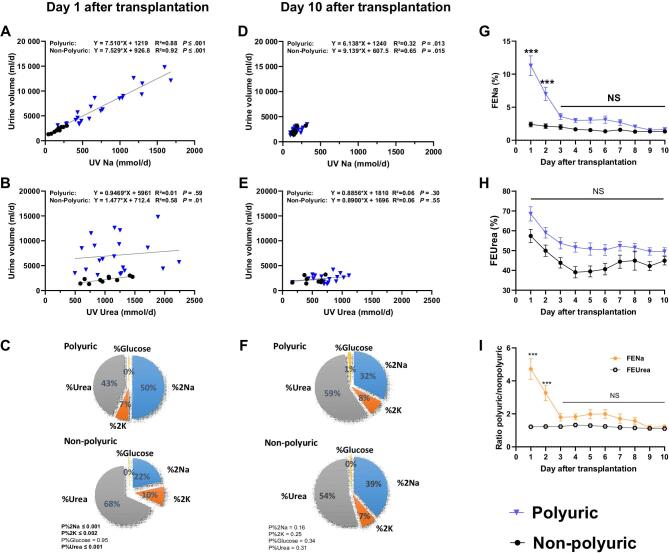
Results: Polyuria occurred in 69.7% of recipients on the first day post-transplantation, independent of residual diuresis, ischemia time, or donor pre-transplantation urine volume. Urine output decreased to normal within 10 days, with no differences in serum creatinine or urinary kidney injury markers between polyuric and non-polyuric patients. Mechanistically, polyuria was driven by sodium-dependent osmotic diuresis, with sodium excretion being the sole decisive driver of early post-transplantation urine volume.
Conclusions: Polyuria after living donor kidney transplantation occurred in nearly 70% of cases without affecting short-term graft function and is explained by sodium-dependent osmotic diuresis. No donor- or recipient-specific predictors could be identified. Careful volume management is crucial in managing this condition.
Keywords: living donor kidney transplantation; osmotic diuresis; polyuria.
© The Author(s) 2025. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
None declared.
Figures

Similar articles
-
Interventions for chronic non-hypovolaemic hypotonic hyponatraemia.Cochrane Database Syst Rev. 2018 Jun 28;6(6):CD010965. doi: 10.1002/14651858.CD010965.pub2. Cochrane Database Syst Rev. 2018. PMID: 29953167 Free PMC article.
-
Glucose-lowering agents for treating pre-existing and new-onset diabetes in kidney transplant recipients.Cochrane Database Syst Rev. 2017 Feb 27;2(2):CD009966. doi: 10.1002/14651858.CD009966.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jul 30;8:CD009966. doi: 10.1002/14651858.CD009966.pub3. PMID: 28238223 Free PMC article. Updated.
-
Catheter-directed therapies for the treatment of high risk (massive) and intermediate risk (submassive) acute pulmonary embolism.Cochrane Database Syst Rev. 2022 Aug 8;8(8):CD013083. doi: 10.1002/14651858.CD013083.pub2. Cochrane Database Syst Rev. 2022. PMID: 35938605 Free PMC article.
-
Home treatment for mental health problems: a systematic review.Health Technol Assess. 2001;5(15):1-139. doi: 10.3310/hta5150. Health Technol Assess. 2001. PMID: 11532236
-
Nitric oxide donors for cervical ripening and induction of labour.Cochrane Database Syst Rev. 2016 Dec 5;12(12):CD006901. doi: 10.1002/14651858.CD006901.pub3. Cochrane Database Syst Rev. 2016. PMID: 27918616 Free PMC article.
References
LinkOut - more resources
Full Text Sources
