

Prediction of First-Onset Cerebral Infarction Risk in Patients with Acute Myocardial Infarction: A Retrospective Cohort Study
- PMID: 40600130
- PMCID: PMC12212101
- DOI: 10.2147/IJGM.S523100
Prediction of First-Onset Cerebral Infarction Risk in Patients with Acute Myocardial Infarction: A Retrospective Cohort Study
Abstract
Background: The occurrence of cerebral infarction significantly increases the risk of major adverse cardiovascular events in patients with acute myocardial infarction (AMI), highlighting the importance of early identification and intervention. Currently, no validated tools exist for individualized risk stratification of cerebral infarction (CI) in patients with AMI.
Objective: This study aimed to identify the most valuable predictors (MVPs) of in-hospital first-onset CI in AMI patients and construct a nomogram for risk stratification.
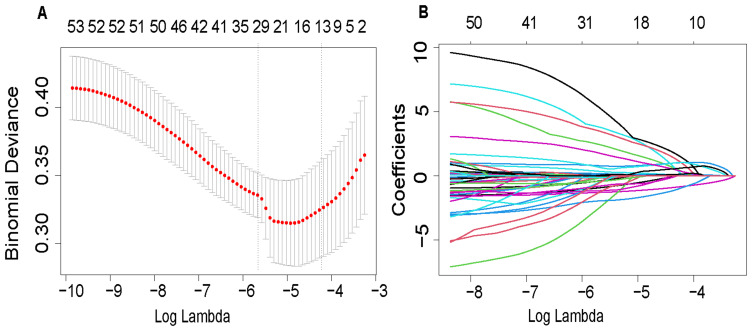
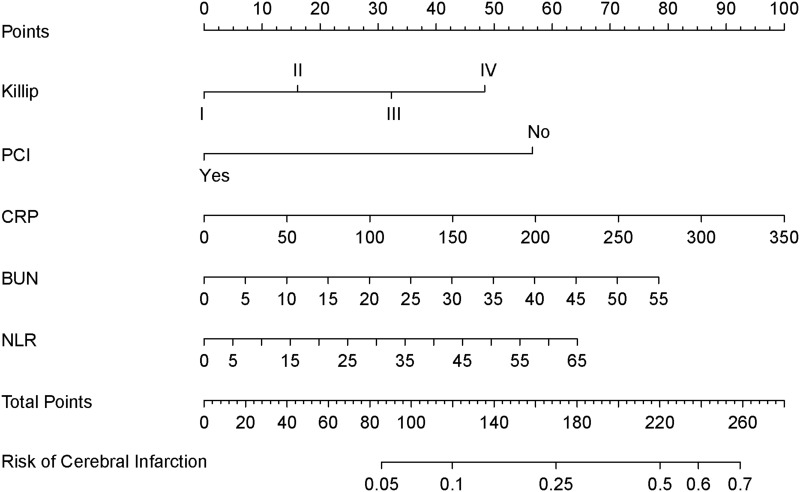
Methods: This retrospective cohort study enrolled 1,350 AMI patients admitted to the Cardiovascular Center of Meizhou People's Hospital between January and December 2022. Clinical characteristics and laboratory parameters were analyzed. Least Absolute Shrinkage and Selection Operator regression (LASSO) was used to select MVPs. The nomogram was developed by integrating coefficients of MVPs from logistic regression, and its discrimination, calibration, and clinical utility were validated in the cohort. The optimal cutoff value of the nomogram probability was determined.
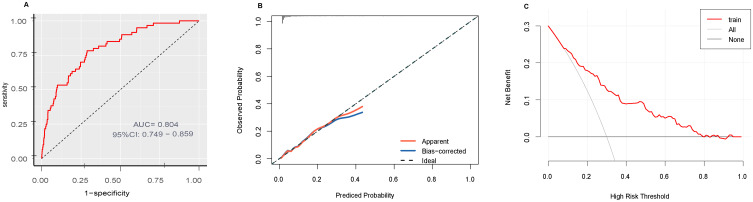
Results: CI occurred in 60 patients (4.44%). MVPs included Killip classification (OR = 1.42, 95% CI 1.05-1.93), PCI therapy (OR = 0.29, 95% CI 0.16-0.51), C-reactive protein (CRP: OR = 1.01, 95% CI 1.00-1.01), blood urea nitrogen (BUN: OR = 1.03, 95% CI 0.99-1.07), and neutrophil-to-lymphocyte ratio (NLR: OR = 1.02, 95% CI 0.99-1.05). The discriminatory ability of the nomogram was up to 0.804(95% CI 0.749-0.859). Additionally, the nomogram showed good calibration and clinical utility in the cohort. Furthermore, the optimal cutoff value of the nomogram probability for distinguishing those who will experience in-hospital first-onset CI was 0.035 (sensitivity 78.3%, specificity 71.1%).
Conclusion: The first nomogram integrating multimodal predictors for discerning AMI patients who will experience in-hospital first-onset CI was developed and validated, which will aid clinicians in clinical decision-making.
Keywords: acute myocardial infarction; cerebral infarction; first-onset; model; nomogram.
© 2025 Zeng et al.
Conflict of interest statement
The authors declare that they have no competing interests in this work.
Figures
Similar articles
-
Retrospective cohort analysis on predicting pulmonary fibrosis in elderly SARS-CoV-2-infected patients.Front Cell Infect Microbiol. 2025 Jun 6;15:1587321. doi: 10.3389/fcimb.2025.1587321. eCollection 2025. Front Cell Infect Microbiol. 2025. PMID: 40546283 Free PMC article.
-
Sex-based differences in inflammatory predictors of outcomes in patients undergoing mechanical thrombectomy: an inverse probability weighting analysis.Ther Adv Neurol Disord. 2025 Jun 21;18:17562864251345719. doi: 10.1177/17562864251345719. eCollection 2025. Ther Adv Neurol Disord. 2025. PMID: 40547862 Free PMC article.
-
A novel nomogram for predicting osteoporosis with low back pain among the patients in Wenshan Zhuang and Miao Autonomous Prefecture of China.Front Endocrinol (Lausanne). 2025 Jun 5;16:1535163. doi: 10.3389/fendo.2025.1535163. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40538801 Free PMC article.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
The comparative and added prognostic value of biomarkers to the Revised Cardiac Risk Index for preoperative prediction of major adverse cardiac events and all-cause mortality in patients who undergo noncardiac surgery.Cochrane Database Syst Rev. 2021 Dec 21;12(12):CD013139. doi: 10.1002/14651858.CD013139.pub2. Cochrane Database Syst Rev. 2021. PMID: 34931303 Free PMC article.
References
-
- Anderson HVS, Masri SC, Abdallah MS, et al. acc/aha key data elements and definitions for chest pain and acute myocardial infarction: a report of the American heart association/American college of cardiology joint committee on clinical data standards. Circul Cardiovasc Quality Outcomes. 2022;15(10). doi: 10.1161/HCQ.0000000000000112 - DOI - PubMed
-
- Improvement NCFC. Executive summary of the 2023 national report on the medical care quality of cardiovascular disease in China. Chin Circul J. 2024;39:625–660. doi: 10.3969/j.issn.1000-3614.2024.07.001 - DOI
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
