

Early Outcomes of Primary Graft Dysfunction Comparing Donation After Circulatory and Brain Death Heart Transplantation: An Analysis of the UNOS Registry
- PMID: 40600382
- PMCID: PMC12216797
- DOI: 10.1111/ctr.70222
Early Outcomes of Primary Graft Dysfunction Comparing Donation After Circulatory and Brain Death Heart Transplantation: An Analysis of the UNOS Registry
Abstract
Background: Primary graft dysfunction (PGD) represents a leading cause of mortality in patients undergoing donation after brain death (DBD) orthotopic heart transplantation (OHT), requiring timely escalation to mechanical circulatory support. There is a lack of nationwide data regarding PGD after donation after circulatory death (DCD). Here, we evaluated the incidence and short-term outcomes of PGD following DCD.
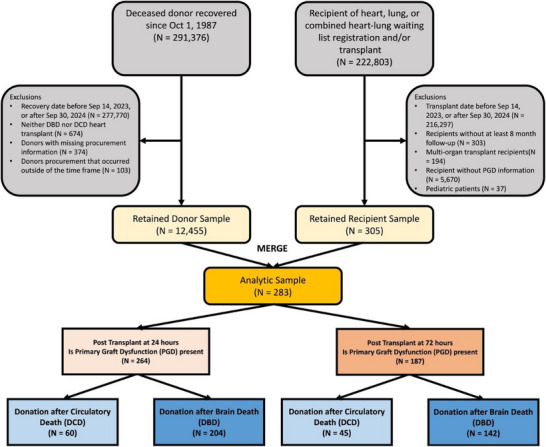
Methods: Using the UNOS registry between 9/2023 and 9/2024, we identified all adult (≥18 years) recipients of OHT. The incidence and outcomes of moderate-severe PGD (24- and 72-h post-transplant) were compared between DCD and DBD. Predictors for mortality after PGD were analyzed using Cox proportional hazard models. 30-day survival was analyzed using the Kaplan-Meier method.
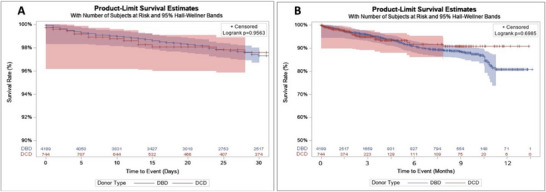
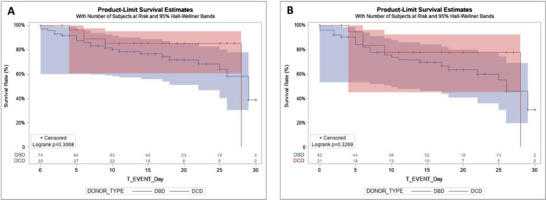
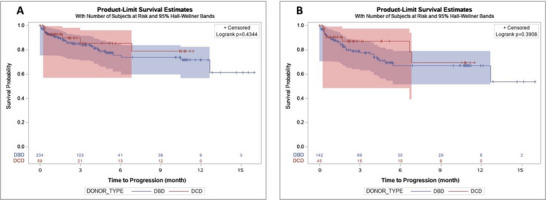
Results: A total of 5017 patients underwent first-time OHT, among whom 762 (15.2%) received DCD hearts. DCD had a significantly higher incidence of PGD at 24- (7.9% vs. 4.8%; p = 0.001) and 72-h (5.9% vs. 3.3%; p = 0.001) compared to DBD. 30-day (p = 0.3068) survival was not different between DCD and DBD patients with PGD. Similarly, for recipients with PGD at 72 h, 30-day (p = 0.327) survival was comparable. At 72 h, DCD recipients were more likely to be supported on ECMO (p = 0.016). Transplanting DCD organs did not impact PGD-associated mortality at 24- (HR 0.72, p = 0.442) and 72-h (HR 0.74, p = 0.457). Postoperative ECMO was associated with decreased risk of PGD-associated mortality in DCD recipients at 24- (p < 0.0001) and 72-h (p < 0.0001).
Conclusions: While PGD rates appear higher in DCD, the associated mortality remains comparable to that of DBD. Early support on ECMO may confer survival benefits in DCD recipients with PGD.
Keywords: donation after brain death; donation after circulatory death; heart transplant; primary graft dysfunction.
© 2025 The Author(s). Clinical Transplantation published by Wiley Periodicals LLC.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Direct procurement with machine perfusion and normothermic regional perfusion in donation after circulatory death heart transplantation.J Thorac Cardiovasc Surg. 2025 Jul;170(1):256-265.e6. doi: 10.1016/j.jtcvs.2024.10.033. Epub 2024 Oct 26. J Thorac Cardiovasc Surg. 2025. PMID: 39490962
-
Impact of donor obesity on outcomes of donation after circulatory death heart transplantation.J Thorac Cardiovasc Surg. 2025 Aug;170(2):594-605.e2. doi: 10.1016/j.jtcvs.2024.12.016. Epub 2024 Dec 24. J Thorac Cardiovasc Surg. 2025. PMID: 39725344
-
Outcomes of Donor-Recipient Size Mismatch in Donation After Circulatory Death Heart Transplantation.Clin Transplant. 2025 Jul;39(7):e70232. doi: 10.1111/ctr.70232. Clin Transplant. 2025. PMID: 40638398
-
Comparisons of liver transplant from DCD outcomes in high-utilization centers versus low-utilization centers in the US: a systematic review and meta-analysis.Front Immunol. 2025 May 9;16:1564551. doi: 10.3389/fimmu.2025.1564551. eCollection 2025. Front Immunol. 2025. PMID: 40416988 Free PMC article.
-
Implementation of donation after circulatory death kidney transplantation can safely enlarge the donor pool: A systematic review and meta-analysis.Int J Surg. 2021 Aug;92:106021. doi: 10.1016/j.ijsu.2021.106021. Epub 2021 Jul 10. Int J Surg. 2021. PMID: 34256169
References
-
- Sabatino M., Vitale G., Manfredini V., et al., “Clinical Relevance of the International Society for Heart and Lung Transplantation Consensus Classification of Primary Graft Dysfunction After Heart Transplantation: Epidemiology, Risk Factors, and Outcomes,” Journal of Heart and Lung Transplantation 36, no. 11 (2017): 1217–1225, 10.1016/j.healun.2017.02.014. - DOI - PubMed
-
- Hull T. D., Crowley J. C., Villavicencio M. A., and D'Alessandro D. A., “Primary Graft Dysfunction in Heart Transplantation: How to Recognize It, When to Institute Extracorporeal Membrane Oxygenation, and Outcomes,” JTCVS Open 8 (2021): 128–133, 10.1016/j.xjon.2021.05.010. Published online May 27. - DOI - PMC - PubMed
-
- Quader M., Hawkins R. B., Mehaffey J. H., et al., “Investigators for the Virginia Cardiac Services Quality Initiative. Primary Graft Dysfunction After Heart Transplantation: Outcomes and Resource Utilization,” Journal of Cardiac Surgery 34, no. 12 (2019): 1519–1525, 10.1111/jocs.14274. - DOI - PubMed
-
- Squiers J. J., Saracino G., Chamogeorgakis T., et al., “Application of the International Society for Heart and Lung Transplantation (ISHLT) Criteria for Primary Graft Dysfunction After Cardiac Transplantation: Outcomes From a High‐Volume Centre,” European Journal of Cardio‐Thoracic Surgery 51, no. 2 (2017): 263–270, 10.1093/ejcts/ezw271. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
