

Combining MRI radiomics, hypoxia gene signature score and clinical variables for prediction of biochemical recurrence-free survival after radiotherapy in prostate cancer
- PMID: 40601075
- PMCID: PMC12367909
- DOI: 10.1007/s11547-025-02037-4
Combining MRI radiomics, hypoxia gene signature score and clinical variables for prediction of biochemical recurrence-free survival after radiotherapy in prostate cancer
Abstract
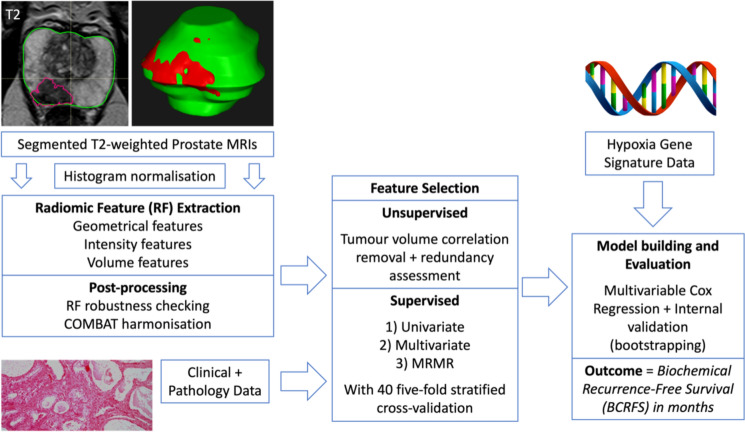
Purpose: To investigate the value of combining MRI radiomic and hypoxia-associated gene signature information with clinical data for predicting biochemical recurrence-free survival (BCRFS) after radiotherapy for prostate cancer.
Methods: Patients with biopsy-proven prostate cancer, hypoxia-associated gene signature scores and pre-treatment MRI who received radiotherapy between 01/12/2007 and 31/08/2013 at two cancer centres were included in this retrospective cohort analysis. Prostate segmentation was performed on axial T2-weighted sequences using RayStation (v9.1). Histogram standardisation was applied prior to radiomic feature (RF) extraction. PyRadiomics (v3.0.1) was used to extract RFs for analysis. Four multivariable Cox proportional hazards BCRFS prediction models using clinical information alone and in combination with RFs and/or hypoxia scores were evaluated using concordance index (C-index) [confidence intervals (CI)]. Akaike Information Criterion (AIC) was used to assess model fit.
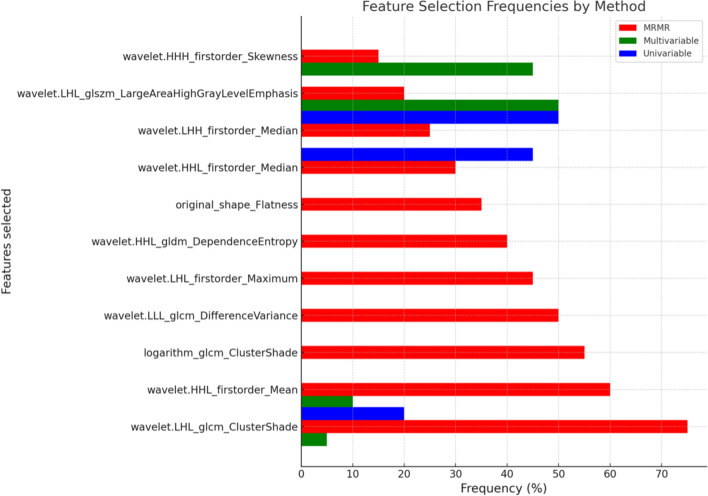
Results: 178 patients were included. The clinical-only model performance C-index score was 0.69 [0.64-0.7]. The combined clinical-radiomics model (C-index 0.70[0.66-0.73]) and clinical-radiomics-hypoxia model (C-index 0.70[0.65-0.73]) both had higher model performance. The clinical-hypoxia model (C-index 0.68 [0.63-0.7) had lower model performance. Based on AIC, addition of RFs to clinical variables alone improved model performance (p = 0.027), whereas adding hypoxia gene signature scores did not (p = 0.625). The selected features of the combined clinical-radiomics model included age, ISUP grade, tumour stage, and wavelet-derived grey level co-occurrence matrix (GLCM) RFs.
Conclusion: Adding pre-treatment prostate MRI-derived radiomic features to a clinical model improves accuracy of predicting BCRFS after prostate radiotherapy, however addition of hypoxia gene signatures does not improve model accuracy.
Keywords: Hypoxia; Magnetic resonance imaging; Prostate cancer; Radiomics; Radiotherapy.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: The authors have no relevant financial or non-financial interests to disclose. Consent to participate: Informed consent was obtained from all individual participants included in the study. Ethical approval: This study was performed in line with the principles of the Declaration of Helsinki. The study was approved by the United Kingdom North West Research Ethics Committee (Validation and qualification of a multiplex hypoxia biomarker for radiotherapy individualisation in prostate cancer study (IRAS 15/NW/0559)). Human or animal rights: Not applicable.
Figures

Similar articles
-
Enhanced ISUP grade prediction in prostate cancer using multi-center radiomics data.Abdom Radiol (NY). 2025 Sep;50(9):4301-4310. doi: 10.1007/s00261-025-04858-3. Epub 2025 Mar 6. Abdom Radiol (NY). 2025. PMID: 40047870 Free PMC article.
-
MRI-Based Radiomics Methods for Predicting Ki-67 Expression in Breast Cancer: A Systematic Review and Meta-analysis.Acad Radiol. 2024 Mar;31(3):763-787. doi: 10.1016/j.acra.2023.10.010. Epub 2023 Nov 2. Acad Radiol. 2024. PMID: 37925343
-
Multimodal MRI radiomics based on habitat subregions of the tumor microenvironment for predicting risk stratification in glioblastoma.PLoS One. 2025 Jun 27;20(6):e0326361. doi: 10.1371/journal.pone.0326361. eCollection 2025. PLoS One. 2025. PMID: 40577371 Free PMC article.
-
Combining multi-parametric MRI radiomics features with tumor abnormal protein to construct a machine learning-based predictive model for prostate cancer.Sci Rep. 2025 Jul 2;15(1):22816. doi: 10.1038/s41598-025-05718-2. Sci Rep. 2025. PMID: 40596249 Free PMC article.
-
Neo-adjuvant and adjuvant hormone therapy for localised and locally advanced prostate cancer.Cochrane Database Syst Rev. 2006 Oct 18;2006(4):CD006019. doi: 10.1002/14651858.CD006019.pub2. Cochrane Database Syst Rev. 2006. PMID: 17054269 Free PMC article.
Cited by
-
Integrative machine learning models predict prostate cancer diagnosis and biochemical recurrence risk: Advancing precision oncology.NPJ Digit Med. 2025 Aug 16;8(1):524. doi: 10.1038/s41746-025-01930-6. NPJ Digit Med. 2025. PMID: 40819002 Free PMC article.
References
-
- Cornford P, van den Bergh RCN, Briers E et al (2024) EAU-EANM-ESTRO-ESUR-ISUP-SIOG guidelines on prostate cancer—2024 update. Part I: screening, diagnosis, and local treatment with curative intent. Eur Urol 86:148–163 - PubMed
-
- Jereczek-Fossa BA, Marvaso G, Zaffaroni M et al (2021) Salvage stereotactic body radiotherapy (SBRT) for intraprostatic relapse after prostate cancer radiotherapy: an ESTRO ACROP Delphi consensus. Cancer Treat Rev 98:102206 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
