

Dry Eye Disease Management Via Technological Methods: A Systematic Review and Network Meta-analysis
- PMID: 40601205
- PMCID: PMC12271009
- DOI: 10.1007/s40123-025-01187-y
Dry Eye Disease Management Via Technological Methods: A Systematic Review and Network Meta-analysis
Abstract
Introduction: In recent years, various technological therapeutic modalities have emerged aiming to target the underlying pathophysiology of dry eye disease (DED).
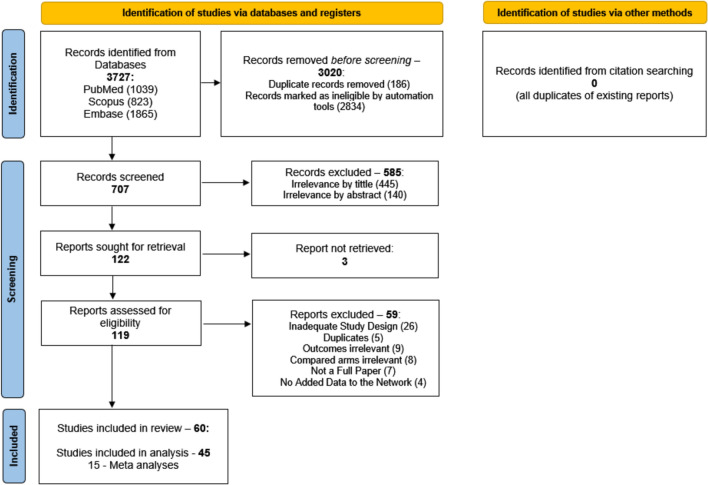
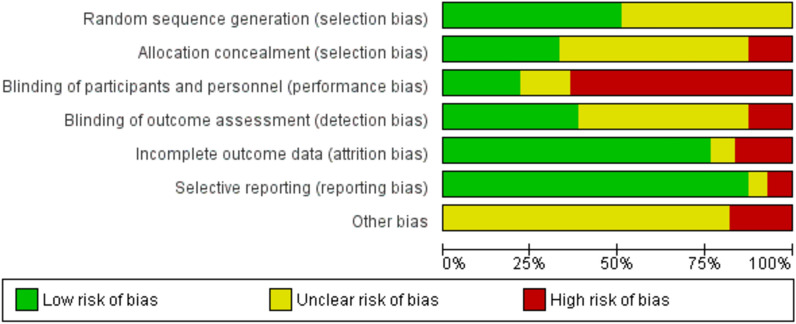
Methods: A systematic search was conducted in PubMed, Scopus, and Embase databases up to July 29, 2023, using predefined search terms related to DED and technological treatments, including intense pulsed light (IPL), LipiFlow, TearCare, iLux, low-level light therapy (LLLT), and acupuncture. Randomized controlled trials (RCTs) evaluating technological interventions for DED with outcome measures for tear secretion, meibomian gland quality, tear break-up time (TBUT), corneal surface health, and symptom scores at 1-2 months post-treatment were included. Data extraction followed PRISMA guidelines. Risk of bias was assessed using Cochrane guidelines. A random-effects frequentist network meta-analysis model was employed, and standardized mean differences (SMDs) were calculated for comparative analyses. P-scores were used to rank treatment efficacy.
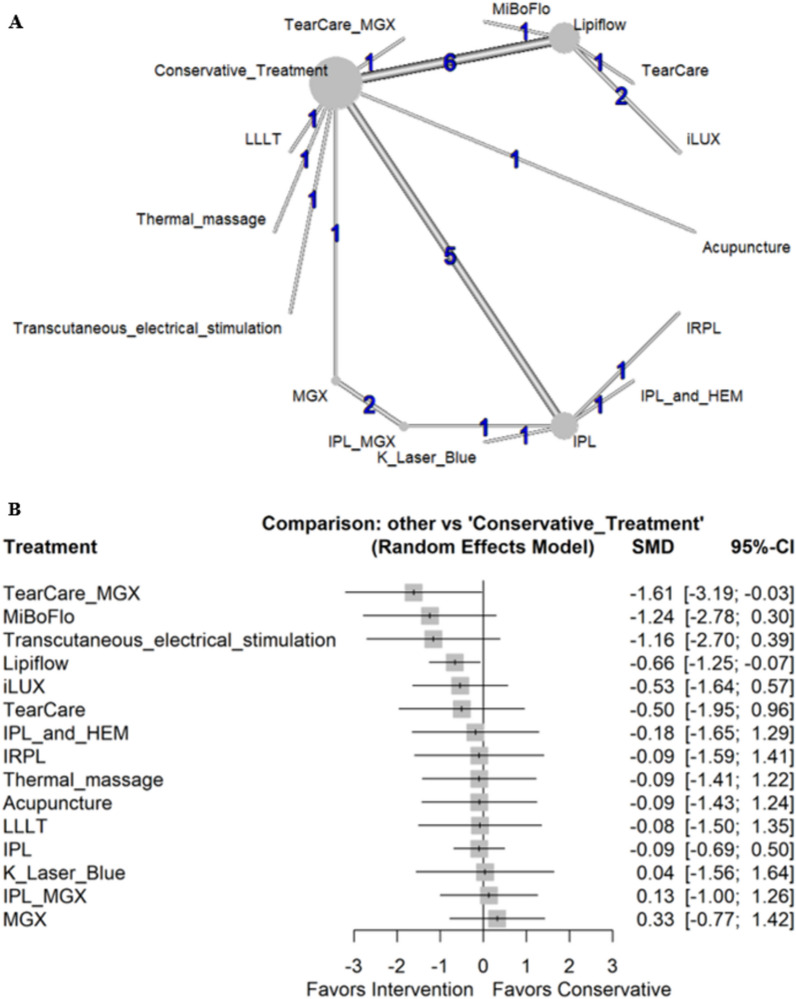
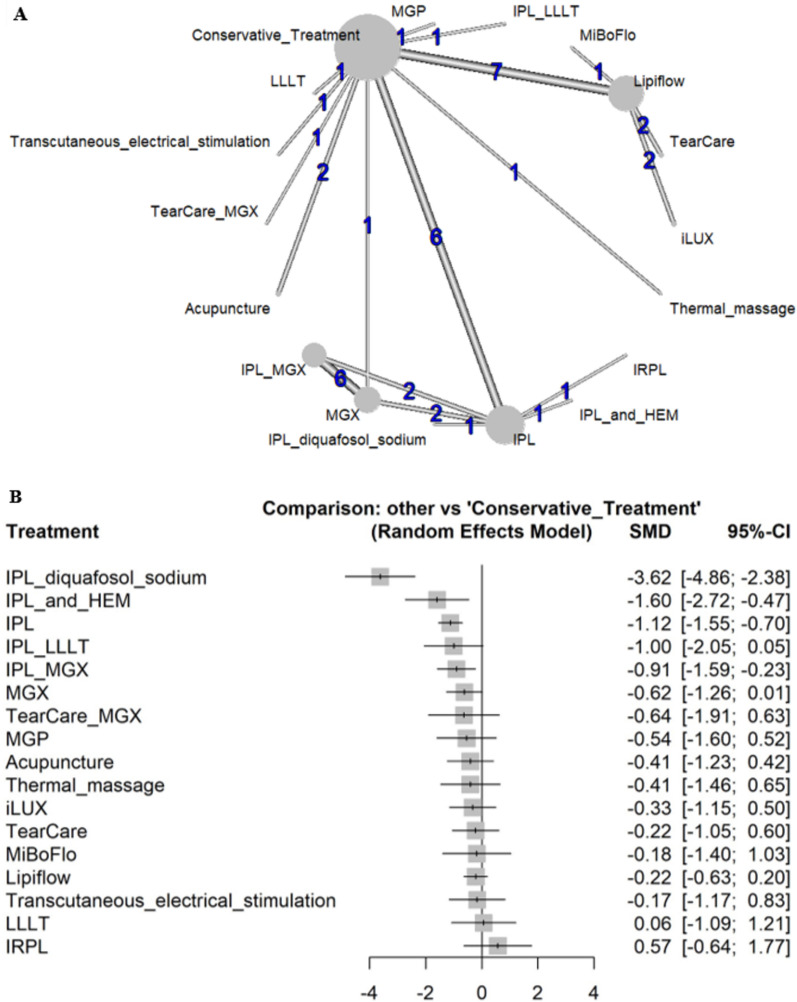
Results: Ultimately, 45 RCTs involving 3455 patients were included. TearCare combined with meibomian gland expression (MGX) demonstrated the highest efficacy for improving meibomian gland secretion (SMD - 10.08, 95% CI - 13.35 to - 6.82). IPL-based treatments, including IPL combined with diquafosol sodium or LLLT, significantly improved TBUT and symptom scores, with IPL alone ranking highest for symptom relief (P-score 0.811). Acupuncture was the only intervention significantly superior to conservative treatment for increasing Schirmer test values (SMD - 0.69, 95% CI - 1.06 to - 0.32). LipiFlow demonstrated modest improvements but was not significantly superior to other technologies.
Conclusions: These findings underscore the potential of advanced technological interventions in the short-term management of DED and support the need for standardized, long-term comparative studies.
Keywords: Dry eye disease; Intense pulsed light; Meibomian gland dysfunction.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: Dror Ben Ephraim Noyman, Clara C. Chan, Joshua C. Teichman, Ruth Lapid-Gortzak, Itamar Arbel, Or Yosefi, Michael Mimouni, and Margarita Safir have nothing to disclose. Ethical Approval: This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors. As such, institutional review board approval and informed consent were not required.
Figures


References
-
- Cutrupi F, De Luca A, Di Zazzo A, Micera A, Coassin M, Bonini S. Real Life Impact of Dye Eye Disease. Semin Ophthalmol. 2023. 10.1080/08820538.2023.2204931. - PubMed
-
- Akpek EK, Amescua G, Farid M, et al. Dry eye syndrome preferred practice pattern®. Ophthalmology. 2019;126(1):P286-p334. 10.1016/j.ophtha.2018.10.023. - PubMed
-
- Cheng SN, Jiang FG, Chen H, Gao H, Huang YK. Intense pulsed light therapy for patients with meibomian gland dysfunction and ocular Demodex infestation. Curr Med Sci. 2019;39(5):800–9. 10.1007/s11596-019-2108-1. - PubMed
-
- Yin Y, Liu N, Gong L, Song N. Changes in the meibomian gland after exposure to intense pulsed light in meibomian gland dysfunction (MGD) patients. Curr Eye Res. 2018;43(3):308–13. 10.1080/02713683.2017.1406525. - PubMed
LinkOut - more resources
Full Text Sources
