

Marginalized Neighborhoods and Health Outcomes in Younger Myocardial Infarction Survivors
- PMID: 40601315
- PMCID: PMC12223890
- DOI: 10.1001/jamanetworkopen.2025.18826
Marginalized Neighborhoods and Health Outcomes in Younger Myocardial Infarction Survivors
Abstract
Importance: Neighborhood characteristics may be independently associated with survival after acute myocardial infarction (AMI).
Objective: To examine the association of living in a marginalized neighborhood with mortality and care for younger AMI survivors (aged <65 years) in a universal health care system.
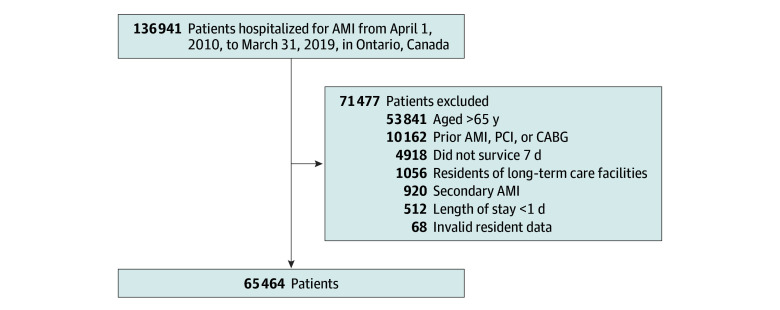
Design, setting, and participants: Population-based retrospective cohort using clinical and administrative databases in Ontario, Canada. Participants were younger patients hospitalized for their first AMI who received invasive evaluation and survived to 7 days after discharge between April 1, 2010, and March 1, 2019. Statistical analysis was performed between May 27, 2022, and March 31, 2025.
Exposures: Neighborhood marginalization, a metric comprising material deprivation, residential instability, and dependency.
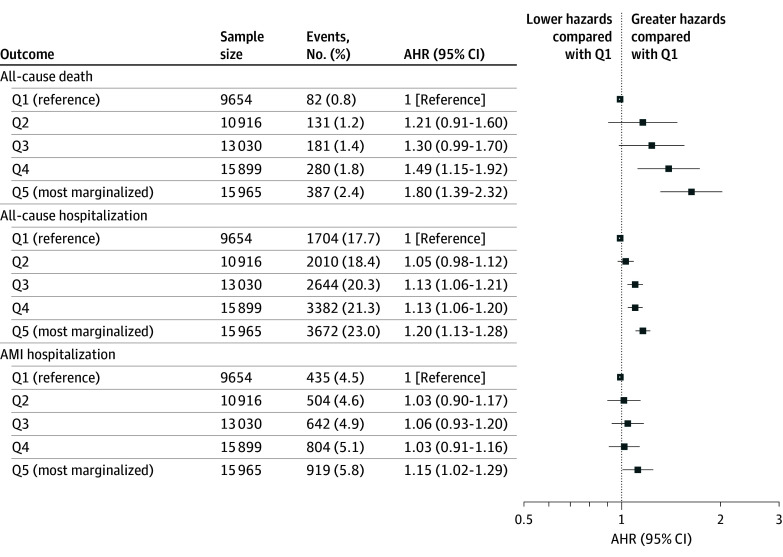
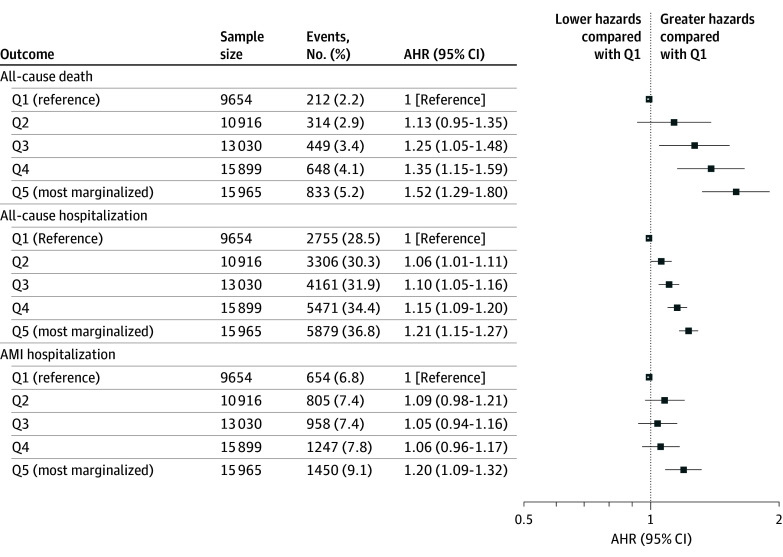
Main outcomes and measures: All-cause death, all-cause hospitalizations, and subsequent AMIs. Proportional hazards regression models were used to quantify the association of marginalization with outcomes over 3 years.
Results: Among 65 464 AMI patients (median age, 56 [IQR, 50-61] years; 22.9% female), increasing neighborhood marginalization was associated with higher rates of mortality beginning 30 days after discharge and persisting over time. At 3 years, mortality rates ranged from 2.2% in the least marginalized neighborhood quintile (Q1) to 5.2% in the most marginalized (Q5). Adjusted hazard ratios for mortality over 3 years of follow-up were significantly higher in patients from marginalized neighborhoods and ranged from 1.13 (95% CI, 0.95-1.35) in Q2 to 1.52 (95% CI, 1.29-1.80) in Q5. Over 1 year, differences were observed between Q1 and Q5 in visits to primary care physicians (Q1, 96.1%; Q5, 91.6%) and cardiologists (Q1, 88.0%; Q5, 75.7%), as well as diagnostic testing.
Conclusions and relevance: In this cohort study of younger AMI survivors with universal health care, living in marginalized neighborhoods was associated with adverse outcomes. The observed differences in health service utilization among marginalized patients warrant further investigation to better understand the underlying structural and systemic factors.
Conflict of interest statement
Figures
Similar articles
-
Neighborhood Disadvantage in a Nationally Representative Sample of Community-Living Older US Adults.JAMA Netw Open. 2024 Dec 2;7(12):e2450332. doi: 10.1001/jamanetworkopen.2024.50332. JAMA Netw Open. 2024. PMID: 39666339 Free PMC article.
-
Examining the Relationship Between Racial, Ethnic, and Economic Residential Segregation and Cigarette Smoking Among a Nationally Representative Sample of Young Adults.Nicotine Tob Res. 2025 May 22;27(6):1016-1024. doi: 10.1093/ntr/ntae277. Nicotine Tob Res. 2025. PMID: 39579345
-
Comparison of Two Modern Survival Prediction Tools, SORG-MLA and METSSS, in Patients With Symptomatic Long-bone Metastases Who Underwent Local Treatment With Surgery Followed by Radiotherapy and With Radiotherapy Alone.Clin Orthop Relat Res. 2024 Dec 1;482(12):2193-2208. doi: 10.1097/CORR.0000000000003185. Epub 2024 Jul 23. Clin Orthop Relat Res. 2024. PMID: 39051924
-
[Volume and health outcomes: evidence from systematic reviews and from evaluation of Italian hospital data].Epidemiol Prev. 2013 Mar-Jun;37(2-3 Suppl 2):1-100. Epidemiol Prev. 2013. PMID: 23851286 Italian.
-
Nutritional interventions for survivors of childhood cancer.Cochrane Database Syst Rev. 2016 Aug 22;2016(8):CD009678. doi: 10.1002/14651858.CD009678.pub2. Cochrane Database Syst Rev. 2016. PMID: 27545902 Free PMC article.
References
-
- Kershaw KN, Magnani JW, Diez Roux AV, et al. ; Council on Quality of Care and Outcomes Research; Council on Epidemiology and Prevention; Council on Clinical Cardiology; Council on Hypertension; Council on Cardiovascular and Stroke Nursing; Council on Peripheral Vascular Disease; and Council on the Kidney in Cardiovascular Disease . Neighborhoods and cardiovascular health: a scientific statement from the American Heart Association. Circ Cardiovasc Qual Outcomes. 2024;17(1):e000124. doi: 10.1161/HCQ.0000000000000124 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
