

Disparities in Treatment and Referral After an Opioid Overdose Among Emergency Department Patients
- PMID: 40601317
- PMCID: PMC12223876
- DOI: 10.1001/jamanetworkopen.2025.18569
Disparities in Treatment and Referral After an Opioid Overdose Among Emergency Department Patients
Abstract
Importance: There is a disproportionately high rate of overdose deaths immediately following an emergency department (ED) visit for opioid overdose. Thus, an improved understanding of disparities in ED treatment and referral is vital. Racial and ethnic disparities in access to naloxone and buprenorphine have been described in the outpatient setting but prevalence in the ED setting remains understudied.
Objective: To examine racial and ethnic disparities in treatment referral rates in ED patients with opioid overdose.
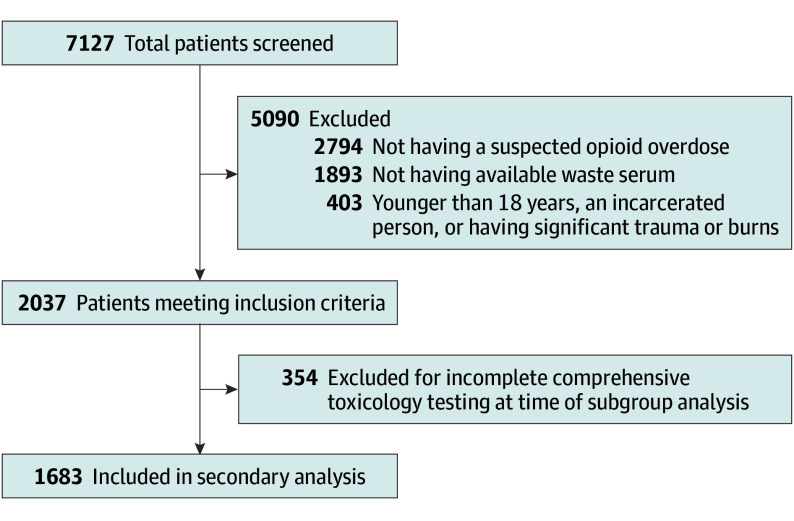
Design, setting, and participants: This is a secondary analysis of a prospective consecutive cohort from the Toxicology Investigators Consortium (TOXIC) Fentalog Study from September 21, 2020, to November 11, 2023. Ten hospital sites were a part of the TOXIC network and participants included ED patients in aged 18 years or older with opioid overdose. Data were analyzed from December 2022 to March 2025.
Exposures: Patient race, ethnicity, sex, and other demographic and clinical factors of interest.
Main outcomes and measures: Study outcomes included the proportion of patients receiving a referral to outpatient addiction care and the proportion receiving a naloxone kit or prescription or buprenorphine prescription at discharge. Descriptive statistics were tabulated, and χ2 and multivariable logistic regression analyses were used to evaluate for differences by race, ethnicity, sex, and other demographic and clinical variables.
Results: In this study, 1683 patients met all inclusion criteria (mean [SD] age, 42.5 [14.5] years; 1221 males [72.6%]; 461 females [27.4%]; 447 Black patients [26.6%]; 63 Hispanic patients [4.3%]; 867 White patients [51.5%]). Of the 1683 included patients, 299 (17.8%) received a referral for outpatient treatment, 713 (42.4%) received a naloxone kit or prescription, and 141 (8.4%) received a buprenorphine prescription. Compared with White patients, Black patients had a decreased adjusted odds ratio (aOR) of outpatient treatment referral (aOR, 0.67; 95% CI, 0.47-0.97). Hospital admission was also associated with increased adjusted odds of outpatient treatment referral (aOR, 3.13; 95% CI, 2.34-4.20). Geographic variation was associated with all primary and secondary outcomes.
Conclusions and relevance: In this study, Black patients were less likely to receive outpatient referrals for OUD. These findings underscore the need for targeted interventions to address racial disparities in ED care for OUD, particularly in enhancing referral processes.
Conflict of interest statement
Similar articles
-
Receipt of Buprenorphine and Naltrexone for Opioid Use Disorder by Race and Ethnicity and Insurance Type.JAMA Netw Open. 2025 Jun 2;8(6):e2518493. doi: 10.1001/jamanetworkopen.2025.18493. JAMA Netw Open. 2025. PMID: 40569592 Free PMC article.
-
Racial and Ethnic Factors and Opioid Use Disorder Treatment After an Emergency Department Visit.JAMA Netw Open. 2025 Jul 1;8(7):e2520661. doi: 10.1001/jamanetworkopen.2025.20661. JAMA Netw Open. 2025. PMID: 40658416 Free PMC article.
-
Disparities by Sex and Race and Ethnicity in Death Rates Due to Opioid Overdose Among Adults 55 Years or Older, 1999 to 2019.JAMA Netw Open. 2022 Jan 4;5(1):e2142982. doi: 10.1001/jamanetworkopen.2021.42982. JAMA Netw Open. 2022. PMID: 35015062 Free PMC article.
-
Do heroin overdose patients require observation after receiving naloxone?Clin Toxicol (Phila). 2017 Feb;55(2):81-87. doi: 10.1080/15563650.2016.1253846. Epub 2016 Nov 16. Clin Toxicol (Phila). 2017. PMID: 27849133
-
Racial and Ethnic Minorities Underrepresented in Pain Management Guidelines for Total Joint Arthroplasty: A Meta-analysis.Clin Orthop Relat Res. 2024 Sep 1;482(9):1698-1706. doi: 10.1097/CORR.0000000000003026. Epub 2024 Mar 18. Clin Orthop Relat Res. 2024. PMID: 38497759
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
