

Preoperative renal functional reserve as a predictor of acute kidney injury in young adults with congenital heart disease
- PMID: 40604226
- PMCID: PMC12223075
- DOI: 10.1038/s41598-025-09461-6
Preoperative renal functional reserve as a predictor of acute kidney injury in young adults with congenital heart disease
Abstract
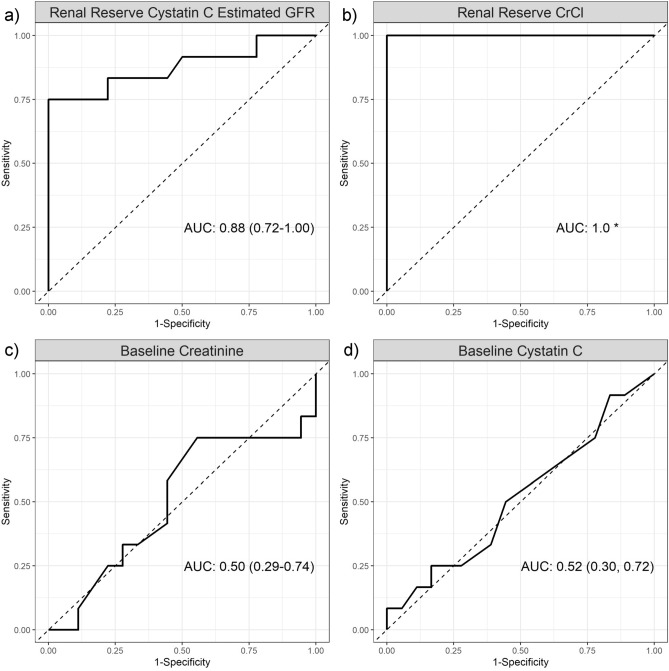
Due to advances in medical and surgical care, there are more adults than children living with congenital heart disease (CHD). Acute kidney injury (AKI) is a common complication following cardiac surgery in patients with CHD, with creatinine lacking sensitivity for early detection. Renal functional reserve (RFR), the kidney's capacity to increase filtration under stress, has emerged as a potential predictor of AKI. Our primary study objective was to evaluate whether preoperative RFR, using both creatinine clearance (CrCl) and cystatin C estimated glomerular filtration rate (eGFR) methods, predicts AKI following cardiopulmonary bypass in young adults with CHD. As a secondary objective, we compared RFR in CHD patients to that of healthy controls. This prospective cohort study included 30 young adults (ages 18-40) with acyanotic CHD and 8 healthy controls with normal baseline kidney function by serum creatinine. Preoperative RFR was measured using CrCl and cystatin C eGFR before and after a protein load. Postoperative AKI was diagnosed using the Kidney Disease Improving Global Outcomes criteria. Twelve (40%) CHD patients developed AKI, exhibiting significantly lower RFR when compared to those without AKI (median CrCl RFR: 9.6 vs. 35.0 mL/min/1.73m2; cystatin C eGFR RFR: 5.5 vs. 11.5 mL/min/1.73m2; P < 0.01). The ROC curve area for AKI prediction was 1.0 (CrCl RFR) and 0.88 (95% CI: 0.72-1.00, cystatin C eGFR RFR). CHD patients had lower RFR than controls (median CrCl: 25.5 vs. 56.4 mL/min/1.73m2, P < 0.01; median cystatin C eGFR: 9.0 vs. 13.5 mL/min/1.73m2, P = 0.03). In conclusion, preoperative RFR accurately predicts AKI in young adults with acyanotic CHD, providing a tool for the identification of high-risk patients and potentially improving perioperative care.
Keywords: Acute kidney injury; Congenital heart disease; Renal functional reserve; Stress GFR.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures



References
-
- Fuhrman, D. Y. et al. Postoperative Acute Kidney Injury in Young Adults With Congenital Heart Disease. Ann. Thorac. Surg.107, 1416–1420 (2019). - PubMed
-
- Bosch, J. P. et al. Renal functional reserve in humans. Effect of protein intake on glomerular filtration rate. Am J Med.75, 943–950 (1983). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
