

STEPWISE management of clinically apparent resistant hypertension in primary care: a cluster randomised controlled trial
- PMID: 40604411
- PMCID: PMC12218076
- DOI: 10.1186/s12875-025-02885-z
STEPWISE management of clinically apparent resistant hypertension in primary care: a cluster randomised controlled trial
Abstract
Background: Clinically apparent resistant hypertension (CARH) is common and a major health problem because it increases the risk of cardiovascular events. We aim to assess whether a stepwise work-up management strategy for patients with CARH in primary care would result in better blood pressure control compared to usual care.
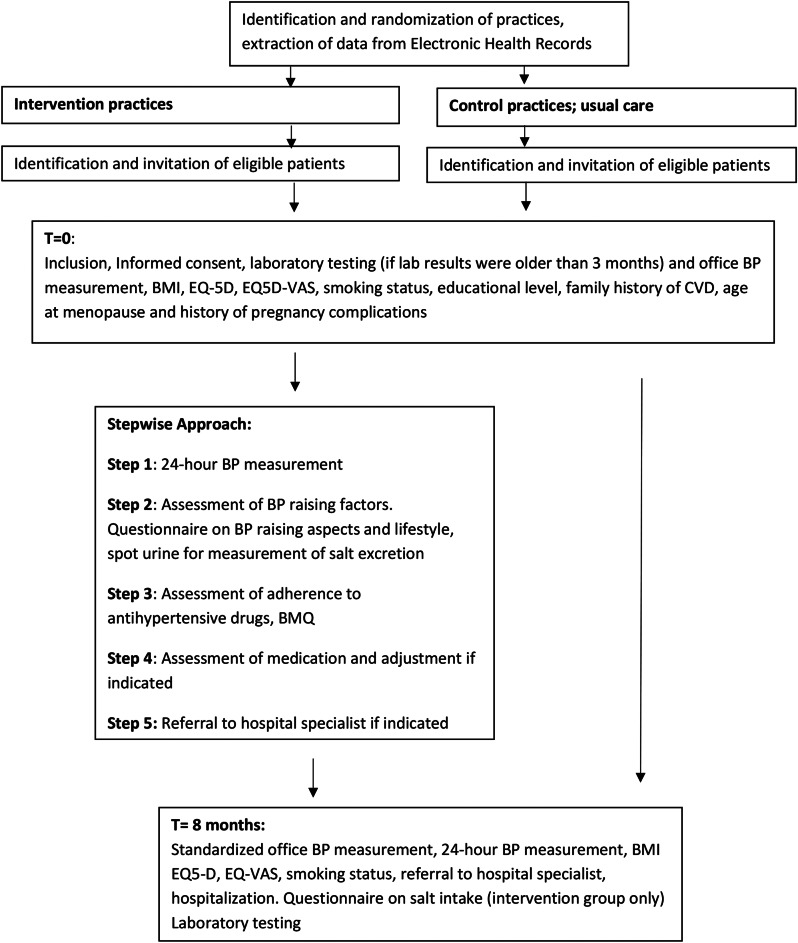
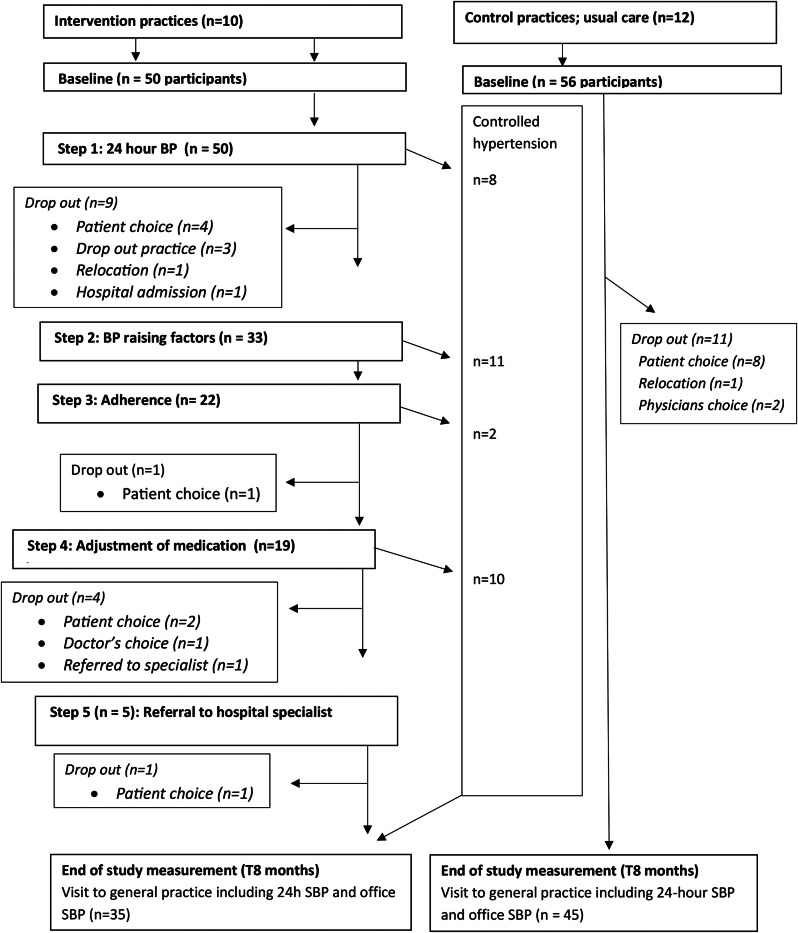
Methods: A pragmatic, cluster-randomised controlled trial (cRCT). General practitioners (GPs) from 22 practices (10 intervention arm; 12 usual care) recruited 106 patients aged 18-80 years who had an office blood pressure (BP) > 140/90 mmHg and were prescribed three or more antihypertensive drugs from different therapeutic classes for three or more months in an adequate dose. This study was conducted between October 2018 and June 2021. The intervention was a stepwise approach comprising of (i) 24-hour blood pressure measurements, (ii) dedicated attention on intake of blood pressure raising compounds, (iii) on lifestyle and on compliance to and (iv) optimalisation of medication, and (v) referral to specialist care, when appropriate. The control group received usual care. Primary outcome was the difference in 24-hours systolic BP between intervention and usual care measured at 8 months after baseline.
Results: Neither 24-hour nor office systolic BP 8 months after baseline significantly differed between intervention and usual care arm: 136.9 mmHg versus 132.6 mmHg (p = 0.15) and 146.1 mmHg versus 147.6 mmHg (p = 0.51), respectively. No significant differences across groups were seen in number of prescribed BP lowering medication: 2.98 versus 3.11, or controlled hypertension after 8 months: 22% versus 28%.
Conclusions: Our results suggest that a pragmatic, structured stepwise approach of CARH does not result in lower 24 h or office BP values compared to usual primary care.
Trial registration: NTR7304 (www.trialregister.nl/trial/7099), May 4th, 2018.
Keywords: Antihypertensives; Cardiovascular disease; Cardiovascular risk; Clinically apparent resistant hypertension; Cluster randomised controlled trial; General practice; Hypertension; Lifestyle; Prevention; Primary care.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The trial was approved by the medical Ethics Committee of the University Medical Center (UMC) Utrecht (NL61553.041.17) and was registered in the Dutch Trial register (reference: NTR7304). All participants signed informed consent to participate. Consent for publication: All participants in the study signed informed consent for publication. Competing interests: The authors declare no competing interests.
Figures
References
-
- Groenland EH, Bots ML, Asselbergs FW, de Borst GJ, Kappelle LJ, Visseren FLJ, Spiering W, UCC-SMART Study Group. Apparent treatment resistant hypertension and the risk of recurrent cardiovascular events and mortality in patients with established vascular disease. Int J Cardiol. 2021;334:135–41. Epub 2021 Apr 29. PMID: 33932429. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- 839110013/The Netherlands Organization for Health Research and Development (ZonMw )
- 839110013/The Netherlands Organization for Health Research and Development (ZonMw )
- 839110013/The Netherlands Organization for Health Research and Development (ZonMw )
- 839110013/The Netherlands Organization for Health Research and Development (ZonMw )
- 839110013/The Netherlands Organization for Health Research and Development (ZonMw )
- 839110013/The Netherlands Organization for Health Research and Development (ZonMw )
- 839110013/The Netherlands Organization for Health Research and Development (ZonMw )
- KF3P0lA/Dutch Kidney foundation
- KF3P0lA/Dutch Kidney foundation
- KF3P0lA/Dutch Kidney foundation
- KF3P0lA/Dutch Kidney foundation
- KF3P0lA/Dutch Kidney foundation
- KF3P0lA/Dutch Kidney foundation
- KF3P0lA/Dutch Kidney foundation
LinkOut - more resources
Full Text Sources
Medical