

Global, regional, and national burden, trends, and inequality analysis of maternal hypertensive disorders (MHD) from 1990 to 2021, and predictions to 2046
- PMID: 40604517
- PMCID: PMC12220113
- DOI: 10.1186/s12884-025-07777-9
Global, regional, and national burden, trends, and inequality analysis of maternal hypertensive disorders (MHD) from 1990 to 2021, and predictions to 2046
Abstract
Background: Maternal hypertensive disorders (MHD) are a leading cause of maternal and fetal mortality, with profound short- and long-term public health impacts. MHD epidemiology remains poorly controlled, and the incidence rate has shown an increase over the past few decades. Therefore, a comprehensive assessment of global burden and prevalence inequalities holds considerable significance for optimizing public health strategies.
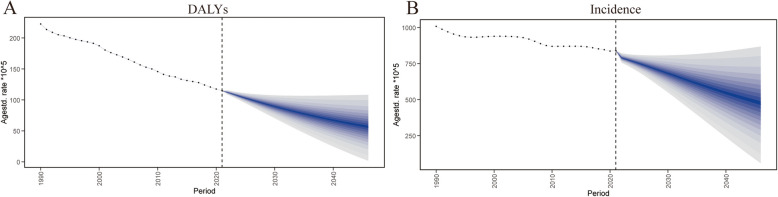
Methods: The global burden and epidemic trend of MHD from 1990 to 2021 were investigated, and the incidence, prevalence, mortality, and disability-adjusted life years (DALYs) were examined utilizing the Global Burden of Disease (GBD). The trends were stratified by age and socio-demographic index (SDI), and further analysis was performed to delve into the correlation between SDI and incidence, prevalence, mortality, and DALYs. Additionally, a Bayesian Age-Period Cohort (BAPC) model was constructed to predict the burden of disease in MHD from 2022 to 2046.
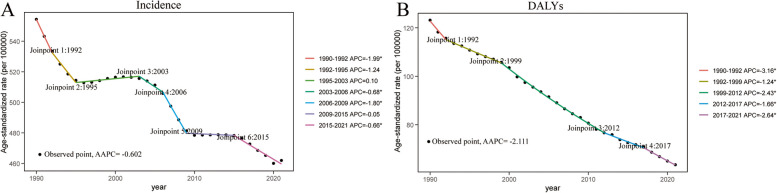
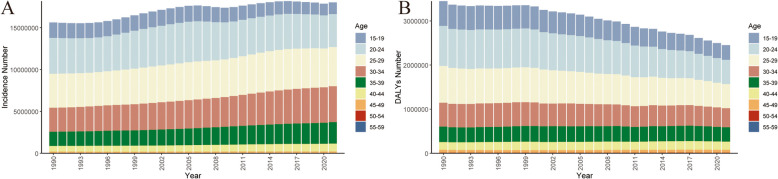
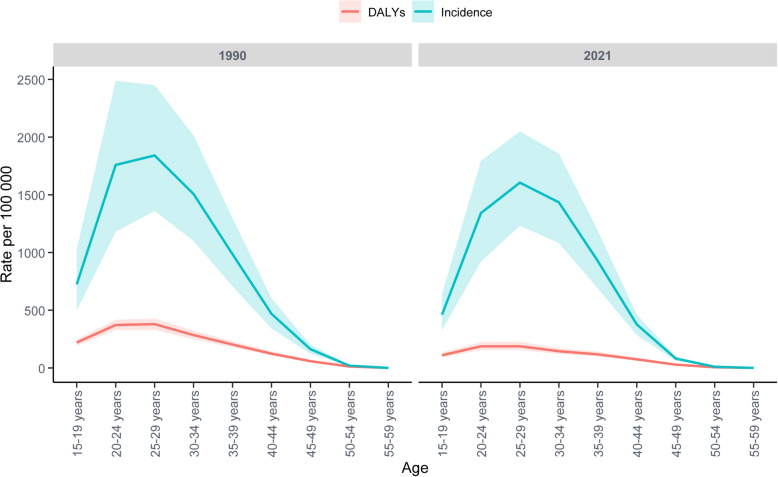
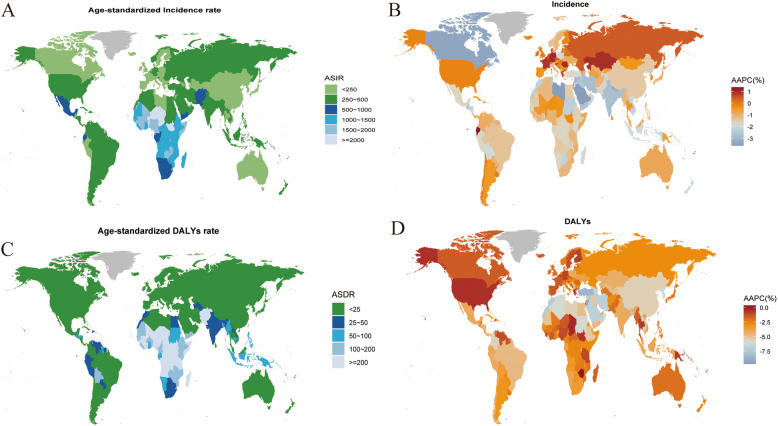
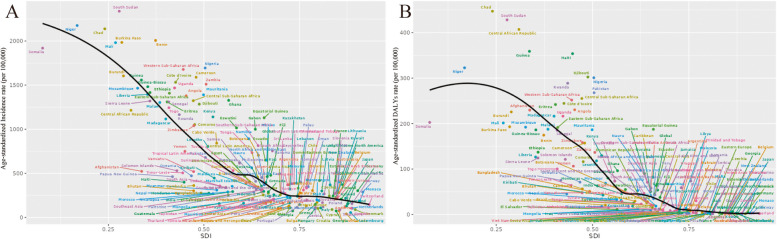
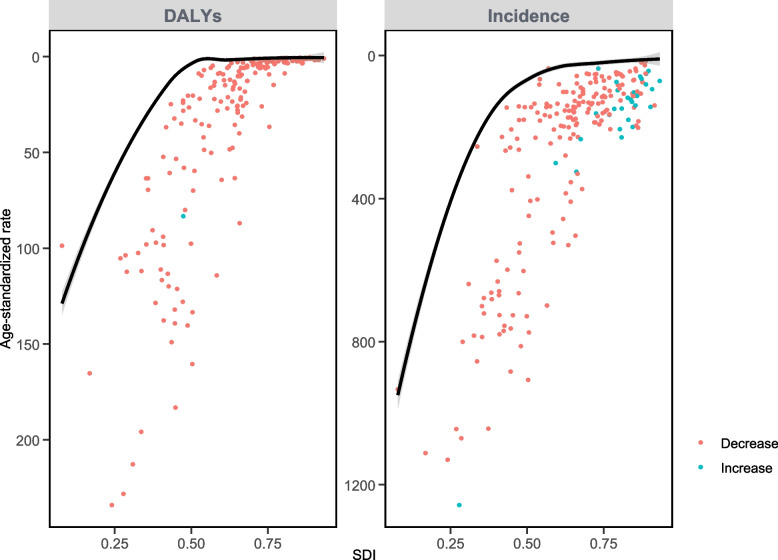
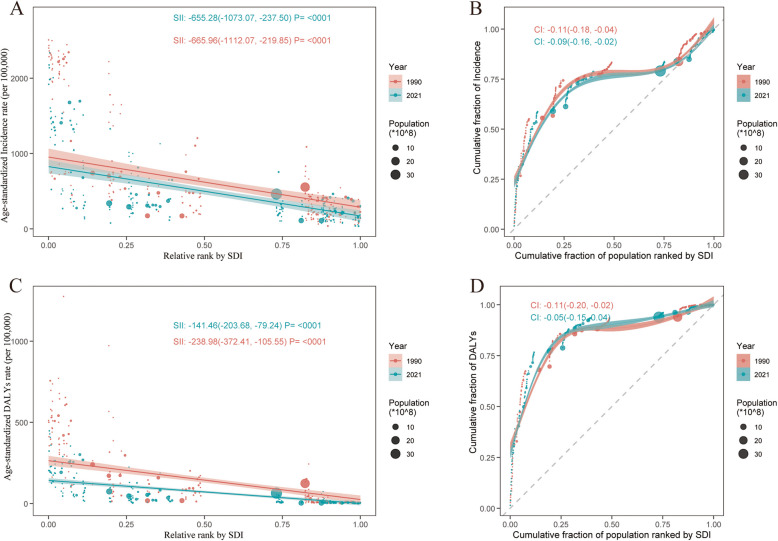
Results: The DALYs induced by MHD decreased significantly from 3.48 million (95% UI, 3.09-3.87 million) in 1990 to 2.47 million (95% UI, 2.08-2.96 million) in 2021, involving an Excess Annual Percentage Change (EAPC) of -2.10. Both the age-standardized DALYs rate (ASDR, AAPC = -2.11) and the age-standardized incidence rate (ASIR, AAPC = -0.60) exhibited evident decreasing trends. The ASDRs of all the age-stratified subgroups decreased as well. Notably, the largest declines were observed in the 20-24 age group with an EAPC of -2.39 (95% UI: -2.56, -2.23). The ASIR exhibited an obvious negative correlation with SDI, and the inequality tended to shrink. Projections for 2046 indicate that global ASDR and ASIR are expected to sustain their downward trajectory. Globally, ASDR in MHD linked to iron deficiency decreased significantly (EAPC = -2.03), with High-middle SDI countries experiencing particularly steep reductions (EAPC = -4.25).
Conclusions: This study performed a comprehensive analysis of the global burden of MHD and observed regional and national inequalities. The investigation also identified a correlation between MHD and SDI, and most regions exhibited an overall declining trend in disease burden. However, further investigations should still be conducted to assist the establishment of public health strategies for MHD prevention.
Keywords: Disability-adjusted life years; Global burden of disease; Hypertension; Incidence; Maternal Hypertensive Disorders.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: All data in this study were collected from GBD database, requiring no additional ethical approval. Consent for publication: All authors approved the publication of this article. Competing interests: The authors declare no competing interests.
Figures
References
-
- Yang L, Huang C, Zhao M, Lee PMY, Zhang C, Yu Y, Xi B, Li J. Maternal hypertensive disorders during pregnancy and the risk of offspring diabetes mellitus in childhood, adolescence, and early adulthood: a nationwide population-based cohort study. BMC Med. 2023;21(1):59. 10.1186/s12916-023-02762-5.PMID:36797785;PMCID:PMC9933265. - DOI - PMC - PubMed
-
- Wang X, Cheng F, Fu Q, Cheng P, Zuo J, Wu Y. Time trends in maternal hypertensive disorder incidence in Brazil, Russian Federation, India, China, and South Africa (BRICS): an age-period-cohort analysis for the GBD 2021. BMC Pregnancy Childbirth. 2024;24(1):731. Published 2024 Nov 8. 10.1186/s12884-024-06931-z. - DOI - PMC - PubMed
-
- Roberts CL, Ford JB, Algert CS, Antonsen S, Chalmers J, Cnattingius S, Gokhale M, Kotelchuck M, Melve KK, Langridge A, Morris C, Morris JM, Nassar N, Norman JE, Norrie J, Sørensen HT, Walker R, Weir CJ. Population-based trends in pregnancy hypertension and pre-eclampsia: an international comparative study. BMJ Open. 2011;1(1):e000101. 10.1136/bmjopen-2011-000101.PMID:22021762;PMCID:PMC3191437. - DOI - PMC - PubMed
-
- Stuart JJ, Tanz LJ, Missmer SA, Rimm EB, Spiegelman D, James-Todd TM, Rich-Edwards JW. Hypertensive disorders of pregnancy and maternal cardiovascular disease risk factor development: an observational cohort study. Ann Intern Med. 2018;169(4):224–32. 10.7326/M17-2740. Epub 2018 Jul 3. PMID: 29971437; PMCID: PMC6601621. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
