

A secondary analysis of cortical atrophy and plasma amyloid β patterns in older patients with cognitive frailty undergoing elective surgery
- PMID: 40604523
- PMCID: PMC12220147
- DOI: 10.1186/s12877-025-05740-z
A secondary analysis of cortical atrophy and plasma amyloid β patterns in older patients with cognitive frailty undergoing elective surgery
Abstract
Background: The etiology of cognitive impairment in frailty may be related to age or to an independent neurodegenerative process, such as Alzheimer's disease (AD). In this secondary analysis, we examine cognitive frailty in patients aged 65 and older undergoing elective surgery, and explore associations with aging- and AD-related cortical atrophy patterns and amyloid β (Aβ) concentrations.
Methods: Cognitive frailty (CF) was defined as the co-occurrence of (pre-)frailty and cognitive impairment (CI). Cognitive performance was assessed using the MMSE and the Cambridge Neuropsychological Teste Automated Battery (CANTAB), while frailty was assessed with a modified version of Fried's frailty phenotype. Aging- and AD-related cortical atrophy patterns were derived from T1-weighted MRI using Freesurfer software. MRI patterns and plasma concentrations of Aβ species 40 and 42 (including Aβ 42/40 ratio) were compared to physically robust, cognitively unimpaired patients using multiple regression analyses and presented as regression coefficient b with 95% confidence intervals.
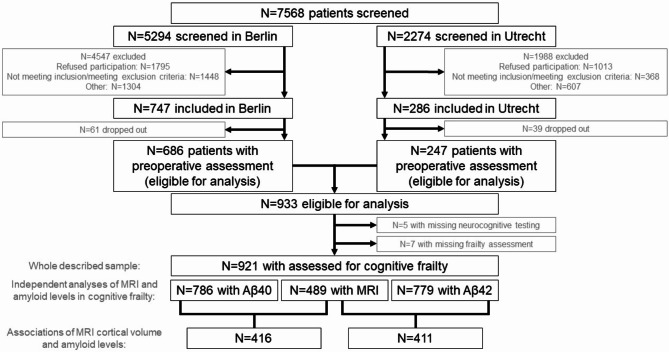
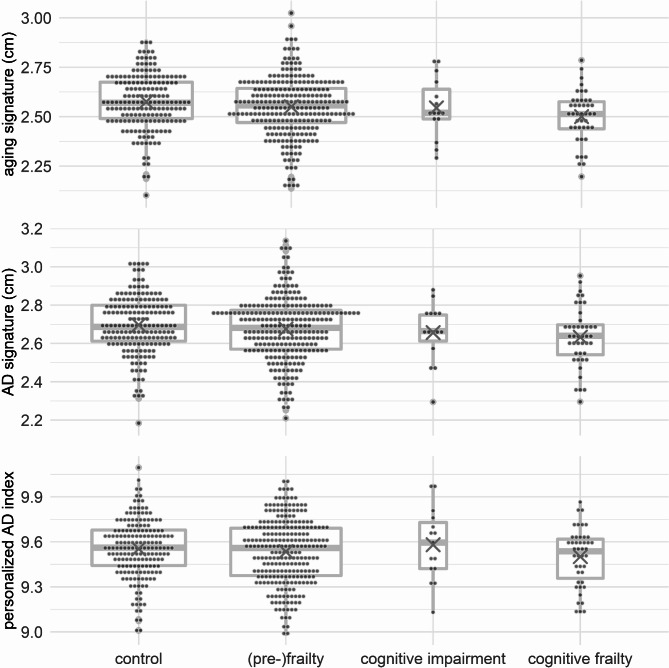
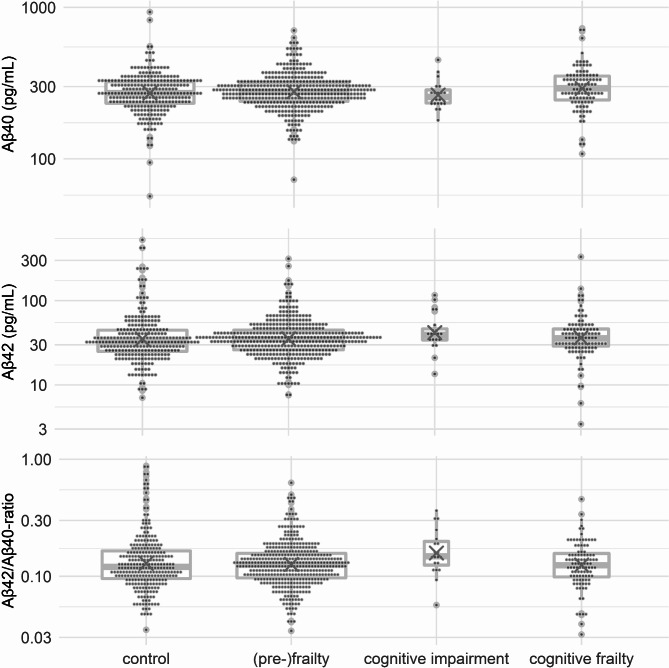
Results: MRI data of N = 489 patients (N = 251 with frailty, N = 15 with CI, N = 43 with CF) and plasma Aβ concentrations of N = 786 patients (N = 400 with frailty, N = 20 with CI, N = 101 with CF) were analyzed. Cognitive frailty was associated with both aging-related and AD-related MRI signatures (bage=-0.070 [-0.113; -0.028], bAD=-0.069 [-0.118; -0.020]). Amyloid β42 was significantly lower in frail patients (b=-0.14 [-0.29; -0.01]), while β42/β40-ratio was lower in patients with frailty (b=-0.11 [-0.21; -0.01]) and cognitive frailty (b=-0.015 [-0.28; -0.03]).
Conclusion: Our results suggest that atrophy in aging- and AD-related cortical regions is associated with cognitive frailty. Plasma amyloid β42/β40-ratios were significantly lower in patients with frailty and cognitive frailty, suggesting that (pre-)frailty in general, rather than cognitive frailty specifically, is associated with AD-like changes. Hence, AD-related pathology seems to be associated with cognitive frailty, but the available data is not sufficient to indicate shared pathomechanisms between AD and cognitive frailty.
Trial registration: ClinicalTrials.gov. Identifier NCT02265263, Date October 15th, 2014.
Keywords: Aging; Amyloidβ; Cognitive frailty; Cortical atrophy; Frailty; MRI.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Written informed consent was obtained from all participants or their proxies. The study was approved by the ethic committees of the Charité – Universitätsmedizin Berlin (ref.: EA2/092/14) and the University Medical Center Utrecht (ref.: 14–469), as well as by their respective data protection officers. The study was conducted in accordance with the Declaration of Helsinki and its amendments and was registered at ClinicalTrials.gov (NCT02265263). Consent for publication: Not applicable. Competing interests: Rudolf Mörgeli, MD: none. Friedrich Borchers, MD: none. Insa Feinkohl, PhD: none. Sophie Piper, PhD: none. Tobias Pischon, MPH, PhD, received grants from the European Commission during the conduct of the study. Arjen Slooter, MD, PhD, received grants from the European Commission during the conduct of the study. Claudia Spies, MD, PhD, received grants from the European Commission during the conduct of the study. During the past 36 months, Prof. Spies received grants from Deutsche Forschungsgemeinschaft, Deutsches Zentrum für Luft- und Raumfahrt e.V., Einstein Stiftung Berlin, Gemeinsamer Bundesausschuss, inner university grants, Projektträger im DLR, Stifterverband, Bundesministerium für Wirtschaft und Klimaschutz, payments by the Georg Thieme Verlag, sponsoring from Dr. F. Köhler Chemie GmbH, Sintetica GmbH, Gemeinsamer Bundesausschuss, Max-Planck-Gesellschaft zur Förderung der Wissenschaften e.V., Stifterverband für die deutsche Wissenschaft, Philipps Electronics Nederland BV, Bundesministerium für Bildung und Forschung/Robert-Koch-Institut. Prof. Spies is involved in patents 15753 627.7 (issued), PCT/EP 2015/067731 (issued), 3 174 588 (issued), 10 2014 215 211.9, 10 2018 114 364.8, 10 2018 110 275.5, 50 2015 010 534.8, 50 2015 010 347.7, 10 2014 215 212.7. Janine Wiebach: none. Georg Winterer, MD, PhD: grants from the European Commission during the conduct of the study. CEO of PharmaImage Biomarker Solutions GmbH Berlin (Germany) and President of its subsidiary Pharmaimage Biomarkers Incl. (Cambridge, MA, USA) and PI Health Solutions GmbH Berlin (Germany). Grants from the Deutsche Forschungsgemeinschaft/German Research Society and from the German Ministry of Health. Norman Zacharias, PhD: none. Florian Lammers-Lietz, MD: personal fees from PharmaImage GmbH during the conduct of the study.
Figures

References
-
- Fried LP, et al. Frailty in older adults: evidence for a phenotype. J Gerontol Biol Sci Med Sci. 2001;56:M146–156. - PubMed
-
- Kelaiditi E, et al. Cognitive frailty: rational and definition from an (I.A.N.A./I.A.G.G.) international consensus group. J Nutr Health Aging. 2013;17:726–34. - PubMed
-
- Canevelli M, Cesari M. Cognitive frailty: what is still missing? J Nutr Health Aging. 2015;19:273–5. - PubMed
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
