

Effect of intradialytic dietary support on nutritional status, muscle strength, and clinical markers in patients on hemodialysis: a cross-sectional study
- PMID: 40604549
- PMCID: PMC12220443
- DOI: 10.1186/s12882-025-04277-y
Effect of intradialytic dietary support on nutritional status, muscle strength, and clinical markers in patients on hemodialysis: a cross-sectional study
Abstract
Background: Intradialytic nutritional support influences nutritional status, muscle strength, and related clinical outcomes in patients undergoing hemodialysis (HD). This study aims to compare the effects of intradialytic nutrition on patient outcomes, malnutrition and sarcopenia risks, and handgrip strength (HGS) in HD patients.
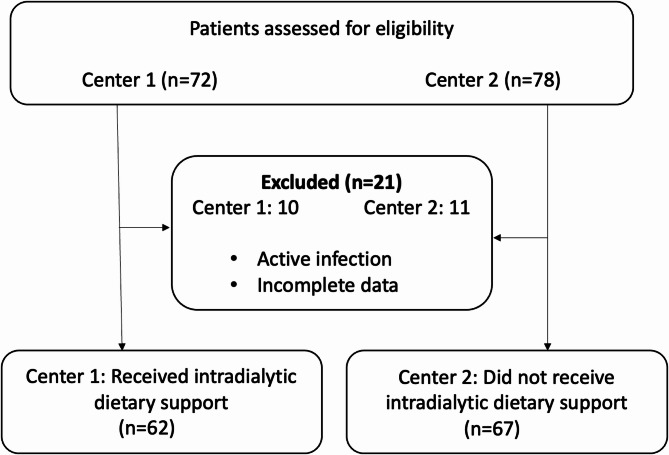
Methods: A cross-sectional study was conducted involving 129 HD patients (62 receiving intradialytic nutritional support and 67 not) from two HD centers located in the same geographic region. Nutritional status was assessed using the MNA-SF, while physical performance was evaluated with SARC-F and HGS. Biochemical markers, including serum albumin, phosphorus, potassium, and hemoglobin (Hb) levels, were measured.
Results: The group receiving intradialytic nutritional support had significantly higher serum albumin (4.0 [3.7-4.2] g/dL vs. 3.5 [3.2-3.7] g/dL; p < 0.001, respectively) and potassium levels (5.6 [5.1-6.2] mmol/L vs. 5.0 [4.7-5.4] mmol/L; p < 0.001, respectively) compared to the group not receiving support. Phosphorus levels were similar between the two groups (4.8 [3.8-6.1] mg/dL vs. 5.3 [4.5-5.2] mg/dL; p = 0.059, respectively). The nutritional support group had lower Hb levels (10.9 ± 1.7 g/dL vs. 11.8 ± 2.0 g/dL; p = 0.008, respectively) and required higher doses of erythropoiesis-stimulating agents (32.0 [24.0-48.0] IU/month×103 vs. 24.0 [18.0-33.0] IU/month×103; p = 0.046, respectively). No significant differences were observed between the groups for MNA-SF and SARC-F scores (13.0 [12.0-14.0] vs. 14.0 [12.0-14.0]; p = 0.608, 5.0 [3.0-7.0] vs. 4.0 [2.0-6.0]; p = 0.053, respectively). The number of patients below the HGS cut-off (27/16 kg) was significantly lower in the nutritional support group (25 [40.3%] vs. 40 [59.7%]; p = 0.028, respectively), and the difference between groups was more pronounced in male patients in terms of median handgrip strength values. The nutritional support group had a higher rate of receiving social financial assistance (45 [72.6%] vs. 37 [55.2%]; p = 0.041) and a higher weekly protein intake.
Conclusion: Intradialytic nutritional support was associated with higher serum albumin levels and handgrip strength, with the latter being more prominent among male patients. However, potassium levels were found to be higher in the nutritional support group, which may present a clinical concern and warrants further monitoring. No significant differences were observed in malnutrition or sarcopenia risk. These findings highlight the potential benefits and limitations of intradialytic nutritional interventions and provide a basis for future prospective studies.
Clinical trial number: Not applicable.
Keywords: Handgrip strength; Hemodialysis; Intradialytic nutritional support; Muscle strength; Nutritional status; Sarcopenia.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by the Van Yuzuncu Yil University Clinical Research Ethics Committee (2024/11 − 02) and conducted in accordance with the 1975 Declaration of Helsinki and its later amendments. All patients enrolled in the study provided informed consent. Consent for publication: Not applicable. Competing interests: The authors declare that they have no competing interests. Outside the submitted work, SM reported receiving support for meeting registration and travel from Amgen and Sanofi Genzyme.
Figures
References
-
- Kurella M, Covinsky KE, Collins AJ, Chertow GM. Octogenarians and nonagenarians starting dialysis in the united States. Ann Intern Med. 2007;146(3):177–83. 10.7326/0003-4819-146-3-200702060-00006. - PubMed
-
- Toker Dincer Z, Dincer MT, Yalin SF, Trabulus S, Seyahi N, Altiparmak MR. Renal and patient outcomes of emergency Hemodialysis in elderly individuals: a retrospective cohort study. Int Urol Nephrol. 2024;56(12):3869–76. 10.1007/s11255-024-04145-y. - PubMed
-
- Carrero JJ, Thomas F, Nagy K, Arogundade F, Avesani CM, Chan M, et al. Global prevalence of Protein-Energy wasting in kidney disease: A Meta-analysis of contemporary observational studies from the international society of renal nutrition and metabolism. J Ren Nutr. 2018;28(6):380–92. 10.1053/j.jrn.2018.08.006. - PubMed
-
- Holvoet E, Vanden Wyngaert K, Van Craenenbroeck AH, Van Biesen W, Eloot S. The screening score of Mini nutritional assessment (MNA) is a useful routine screening tool for malnutrition risk in patients on maintenance dialysis. PLoS ONE. 2020;15(3):e0229722. 10.1371/journal.pone.0229722. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
