

Traditional vs. orthodontic extraction of impacted teeth related to the inferior alveolar nerve: a randomized control trial
- PMID: 40604669
- PMCID: PMC12224594
- DOI: 10.1186/s12903-025-06402-7
Traditional vs. orthodontic extraction of impacted teeth related to the inferior alveolar nerve: a randomized control trial
Abstract
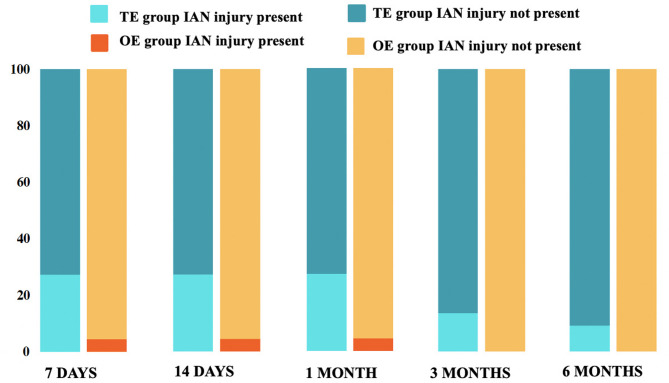
Background: The aim of this prospective randomized controlled trial was to compare the effects of orthodontic and traditional extraction methods on nerve injury following the extraction of impacted third molars close to the inferior alveolar nerve and to demonstrate the impact of factors such as gender, age, systemic diseases, the side of the third molar, its position, and classification on nerve recovery.
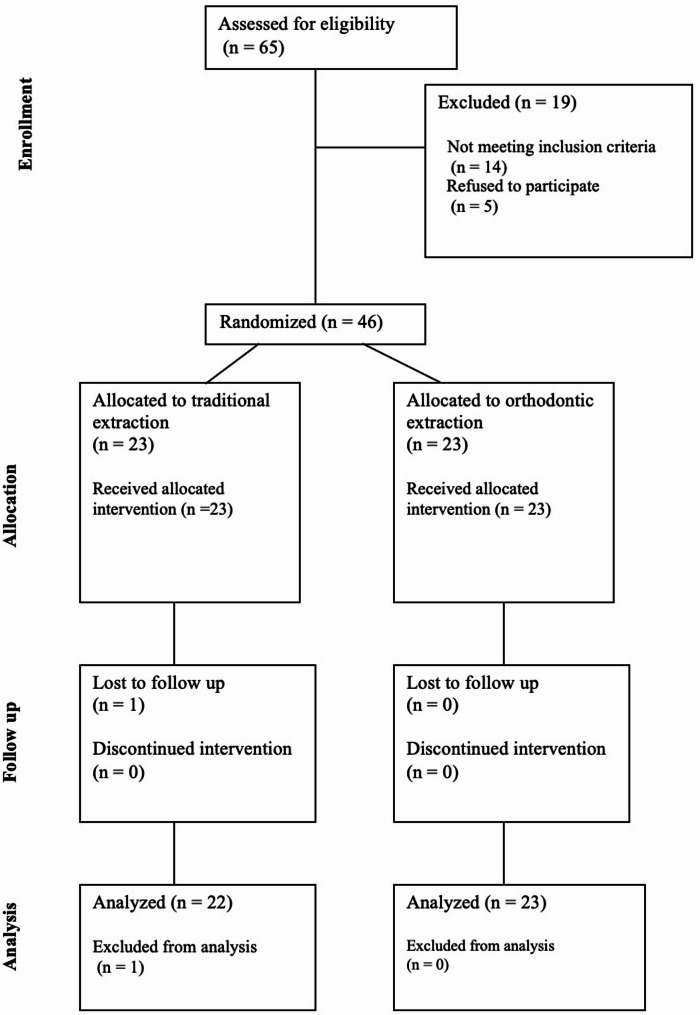
Methods: Patients with impacted third molars close to the inferior alveolar nerve and an indication for impacted third molar extraction were included in the study. The patients were divided into two groups according to the surgical approach to be applied.
Results: Preoperative 2-point discrimination (2PD) test values, as well as postoperative 2PD test and visual analog scales (VAS) values on the 7th day, 14th day, and 1st, 3rd, and 6th months, were compared. In the traditional extraction group, the results of the 2PD test were statistically significantly higher on the 7th day, 14th day, 1 month, and 3 months compared to the orthodontic extraction group (P < 0.05). Sex, age, systemic disease, M3 side, position, and classification had no statistically significant effect on nerve recovery (P > 0.05).
Conclusions: The orthodontic extraction was found to be safer than traditional extraction in terms of nerve injury for high-risk M3s.
Clinical trial registration: This study was registered on www.
Clinicaltrials: govin13/02/2024 .
Clinical trial number: NCT06270784.
Keywords: Impacted tooth; Inferior alveolar nerve; Mandibular nerve injuries; Orthodontic extrusion; Third molar; Tooth extraction.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The present study was performed according to the guidelines of the Helsinki Declaration and complied with the CONSORT guidelines. Ethical approval was obtained from Marmara University Faculty of Medicine Clinical Research Ethical Commitee (IRB Approval No. 09.2024.122). Every patient signed a written informed consent form. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures


Similar articles
-
Surgical removal versus retention for the management of asymptomatic disease-free impacted wisdom teeth.Cochrane Database Syst Rev. 2016 Aug 31;(8):CD003879. doi: 10.1002/14651858.CD003879.pub4. Cochrane Database Syst Rev. 2016. Update in: Cochrane Database Syst Rev. 2020 May 4;5:CD003879. doi: 10.1002/14651858.CD003879.pub5. PMID: 27578151 Updated.
-
Comparison of two surgical techniques for the extraction of mandibular horizontally impacted third molars near the mandibular canal: the displacement reduction method and the away-from-nerve method.Clin Oral Investig. 2025 May 7;29(6):287. doi: 10.1007/s00784-025-06366-6. Clin Oral Investig. 2025. PMID: 40329123
-
Orthodontic Extraction of High-Risk Impacted Mandibular Third Molars in Close Proximity to the Mandibular Canal: A Systematic Review.J Oral Maxillofac Surg. 2015 Sep;73(9):1672-85. doi: 10.1016/j.joms.2015.03.031. Epub 2015 Mar 24. J Oral Maxillofac Surg. 2015. PMID: 25882437
-
Analysis of clinical and radiographic outcomes at least 5 years after coronectomy for deeply impacted mandibular third molars.J Stomatol Oral Maxillofac Surg. 2025 Sep;126(4S):102188. doi: 10.1016/j.jormas.2024.102188. Epub 2024 Dec 4. J Stomatol Oral Maxillofac Surg. 2025. PMID: 39642997
-
Benefits of Coronectomy in Lower Third Molar Surgery: A Systematic Review and Meta-analysis.J Oral Maxillofac Surg. 2024 Jan;82(1):73-92. doi: 10.1016/j.joms.2023.09.024. Epub 2023 Oct 6. J Oral Maxillofac Surg. 2024. PMID: 37925166
References
-
- Steel BJ, Surendran KSB, Braithwaite C, Mehta D, Keith DJW. Current thinking in lower third molar surgery. Br J Oral Maxillofac Surg. 2022;60(3):257–65. 10.1016/j.bjoms.2021.06.016. - PubMed
-
- Flanagan D. Forced extrusion for removal of impacted third molars close to the mandibular Canal. Revista Española De Cirugía Oral Y Maxilofacial. 2012;34:25. 10.1016/j.maxilo.2011.10.003.
-
- Gencheva A, Georgiev T, Arnautska H, Ivanova G, Nogalchev K. Orthodontic extrusion followed by a surgical extraction of high-risk lower third molar: case report. Scripta Scientifica Medicinae Dentalis. 2016;2(2):33–8. 10.14748/ssmd.v2i2.1814.
-
- Bataineh AB. Sensory nerve impairment following mandibular third molar surgery. J Oral Maxillofac Surg. 2001;59(9):1012–7. 10.1053/joms.2001.25827. discussion 1017. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
