

Short-term impact of tirzepatide on metabolic hypogonadism and body composition in patients with obesity: a controlled pilot study
- PMID: 40604795
- PMCID: PMC12220628
- DOI: 10.1186/s12958-025-01425-9
Short-term impact of tirzepatide on metabolic hypogonadism and body composition in patients with obesity: a controlled pilot study
Abstract
Background: Tirzepatide (TZP), a dual agonist of glucose-dependent insulinotropic peptide (GIP) and glucagon-like peptide-1 (GLP-1) receptors, has recently been introduced in Italy for the treatment of obesity. Obesity is frequently associated with metabolic hypogonadism, which is characterized by low testosterone levels and normal low levels of gonadotropin. This condition exacerbates metabolic dysfunction and increases the risk of type 2 diabetes mellitus (DM). This study aims to evaluate the effects of TZP on metabolic hypogonadism in patients with obesity.
Methods: Male patients with obesity and metabolic hypogonadism were enrolled. Exclusion criteria included recent use of medications for hypertension, dyslipidemia, DM, anti-androgens, or hyperprolactinemia. All participants followed a hypocaloric diet and engaged in 20 min of daily brisk walking. Patients were allocated to one of the following treatment groups: Group A received 2.5 mg of TZP weekly for the first month, with the dose increased to 5 mg from the second month; Group B received no pharmacological treatment: Group C received transdermal testosterone. Clinical evaluations were conducted at 2 months including assessment of body composition, the Binge Eating Scale (BES), 5-item International Index of Erectile Function (IIEF-5) questionnaire to evaluate erectile dysfunction (ED), and serum levels of luteinizing hormone (LH), follicle-stimulating hormone (FSH), sex hormone-binding globulin (SHBG), total testosterone (TT), and 17β-estradiol (E2). Free (fT) and bioavailable testosterone (bioT) were calculated using the Vermeulen formula.
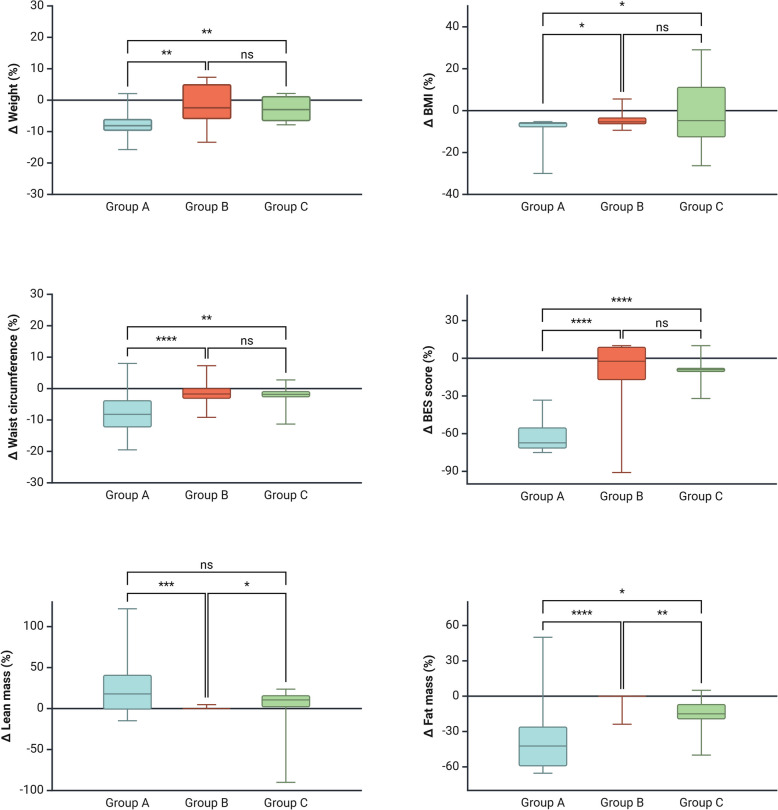
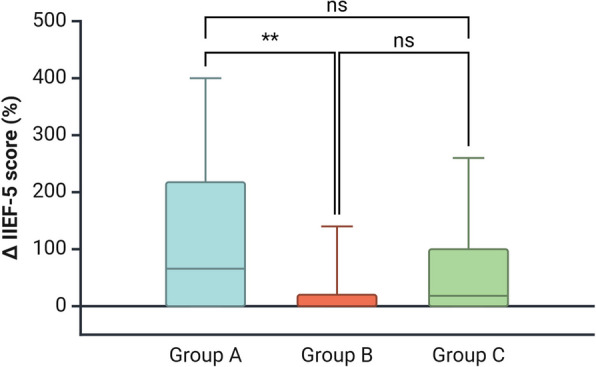
Results: A total of 83 patients with obesity (mean age 55.3 ± 5.5 years) were included in the study, divided into three groups: Group A (28 patients, mean age 56.3 ± 4.7 years), Group B (30 patients, mean age 55.1 ± 5.2 years), and Group C (25 patients, mean age 54.0 ± 6.5 years). At baseline, significant differences were observed in waist circumference (WC), which was higher in Group B, as well as in the BES score, lean mass (LM), and serum LH levels, all of which were higher in Group A. After 2 months, Group A showed significantly greater reductions in body weight, WC, BES score, and fat mass, along with a notable increase in LM and IIEF-5 score compared to Groups B and C. Additionally, Group A exhibited significantly higher serum levels of LH, FSH, SHBG, TT, fT, and bioT, while E2 levels were significantly lower than both Groups B and C.
Conclusion: The results of this study suggest that TZP is effective in improving both metabolic parameters, ED, and gonadal hormone levels in patients with obesity and metabolic hypogonadism. These findings position TZP as a promising treatment for obese patients with functional hypogonadism arising from metabolic-related alterations.
Keywords: Body composition; Fat mass; Gonadotropins; Metabolic hypogonadism; Testosterone; Tirzepatide.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study protocol was carried out in accordance with the ethical principles of the Declaration of Helsinki and its subsequent amendments. Ethical approval was waived as the procedures that patients underwent are standard components of routine clinical practice, and no participants were subjected to any experimental interventions. All participants provided informed consent for the use of their personal and clinical data. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

References
-
- Berg J, Nauman J, Wisløff U. Normative values for body composition in 22,191 healthy Norwegian adults 20–99 years: The HUNT4 study. Prog Cardiovasc Dis. 2024;85:82–92. 10.1016/j.pcad.2024.06.002. Epub 2024 Jun 24. PMID: 38925258. - PubMed
-
- Bhasin S, Brito JP, Cunningham GR, Hayes FJ, Hodis HN, Matsumoto AM, Snyder PJ, Swerdloff RS, Wu FC, Yialamas MA. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2018;103(5):1715–44. 10.1210/jc.2018-00229. PMID: 29562364. - DOI - PubMed
-
- Corona G, Goulis DG, Huhtaniemi I, Zitzmann M, Toppari J, Forti G, Vanderschueren D, Wu FC. European Academy of Andrology (EAA) guidelines on investigation, treatment and monitoring of functional hypogonadism in males: Endorsing organization: European Society of Endocrinology. Andrology. 2020;8(5):970–87. 10.1111/andr.12770. Epub 20 Mar 2020 PMID: 32026626. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
